
Tick tock
 There was Fort Hood in 2009, where 13 people were killed in a shooting spree. Then there was the rampage at Sandy Hook Elementary in 2012, where 27, mostly children, died. Recently, a lone gunman at an Orlando nightclub killed 49 people. The list goes on and on.
There was Fort Hood in 2009, where 13 people were killed in a shooting spree. Then there was the rampage at Sandy Hook Elementary in 2012, where 27, mostly children, died. Recently, a lone gunman at an Orlando nightclub killed 49 people. The list goes on and on.
Over the last decade alone, 538 people have been killed in mass shootings in the U.S. That doesn’t include the multitude of victims of other mass violent, deadly crimes.
Then there are everyday injuries that cause trauma and death: the preschooler playing with a knife that accidentally nicks an artery. The carpenter working with a power saw that slips.
Trauma is the leading cause of death of children, and bleeding is a major preventable cause. It can take as little as five minutes for a person to bleed to death. But simple steps can save lives, and these steps are being taught to emergency personnel and medical professionals so that they can, in turn, empower bystanders to become lifesavers.
It’s like modern-day CPR training, said Kaori Tanaka, D.O., M.S.P.H., assistant professor of emergency medicine. Fear of the unknown prevents many people from being proactive in a bleeding control situation, just as years ago, before widespread CPR training, people didn’t know how to respond to a person in cardiac arrest.
“Once people are trained, they know what to do and have a higher likelihood of being able to act,” Dr. Tanaka said.
Following the Sandy Hook tragedy, the American College of Surgeons in 2013 gathered a panel of physicians, law enforcement and military personnel, and federal agency leaders. They determined that modern American life features a new reality—one where active shooter/mass casualty events happen often enough that people should be better prepared.
“As our experience with these events has accumulated,” the report stated, “it has become clear that longstanding practices of law enforcement, fire/rescue and EMS responses are not optimally aligned to maximize victim survival.”
Ways to improve survival already exist, but they are underutilized, the report found. “While efforts to isolate or stop the active shooter remain paramount, early hemorrhage control is critical to improving survival.”
Dubbed the Hartford Consensus, the group met four more times and developed policies and procedures to improve the care of trauma patients based on lessons learned in the wars in Iraq and Afghanistan. Then, in 2015, the White House launched the “Stop the Bleed” campaign to better prepare the public to save lives by raising awareness of basic ways to stop life-threatening bleeding following everyday emergencies, and man-made and natural disasters.
“The world has experienced its share of natural disasters and high-casualty incidents,” said Ronald Stewart, M.D., professor and chair of the Department of Surgery and chair of the American College of Surgeons’ Committee on Trauma.
“Under these circumstances, emergency services are often spread thin, with multiple individuals with injuries requiring treatment immediately.”
The National Association of Emergency Medical Technicians and the trauma committee joined forces to establish the B-Con Course, short for bleeding control, which trains people on managing bleeding under time-sensitive circumstances before trained responders can arrive. The curriculum has been taught multiple times at the university and across South Texas by UT Health San Antonio and University Health System instructors. It is overseen by the Committee on Trauma.
Bringing the training to campus was about creating momentum for this initiative based on unique challenges that are faced in the 27,000-square-mile South Texas region, Dr. Stewart said. Given its size and geography, it may take longer for emergency responders to arrive to outlying areas.
“In almost any community, it is likely to take more than five minutes to arrive on the scene before someone with trauma can be treated, and in that five minutes, the person can die,” he said. “That is where a trained bystander can really make a difference.”
Currently, the course is offered to the public through instructors in the Division of Trauma & Emergency Surgery, and emergency medicine and emergency health sciences departments. The curriculum, running about an hour long, is focused on the recognition of life-threatening bleeding and appropriate medical treatment. Participants learn how to control bleeding with direct pressure and when and how to apply a tourniquet. They learn how to pack the wound and how to identify injuries to the chest or abdomen, and understand why these victims need immediate hospital transport.
The goal is to create as many instructors as possible so that they can, in turn, teach others and spread knowledge of life-saving techniques in an emergency.
San Antonio is a perfect place to roll out the program, Dr. Stewart said. The city has local expertise in trauma and bleeding control, and “there is the largest military medical presence anywhere in the world,” he said. “It is also surrounded by ranches and large spaces, where hunting and work-related injuries often occur.”
An added bonus, he said, is the community’s willingness to help others.
“The more we can spread this knowledge, the more potential we have for saving lives,” he said.

Essay: House call
at the UT Health Cancer Center.
Caring for people who have cancer does not stop when treatments stop.
Thirty-two years ago, as a hematology-oncology doctor in training at Boston City Hospital, oncology nurses were my primary teachers who influenced me the most about caring for the terminally ill. They showed me what the impact would be on a patient and the family if we went to see them when they could no longer come to the clinic or hospital. Making a visit to see a patient at home is a truly humbling experience, and I have tried to make time to do this, knowing that it reinforces in full measure what it truly means to be a physician.
Burnet, Texas: If you go to Burnet, you will drive through the Hill Country that Texans dearly love, the land of Lyndon Johnson, the Pedernales, stunning vistas. The directions said: “281 to 29 and left into our ranch with the cedar post gates and the cattle guard, and then I’m sorry but a 2-mile dirt road up to our house.” Renal cancer had blown through everything, and the architect lay dying in a home he had designed and built on a hill. “See those beams?” he said, pointing straight up as I sat by his bedside. “I recycled them from a house that was torn down. I was green before it was cool to be green.” On my way out, his wife pointed to Lake Buchanan in the distance, and leaned against my car. A long pause, and then she said, “I know,
I know. One day at a time, right?”
William Carlos Williams, doctor, writer and poet, walked all over Paterson, New Jersey, to see his patients at odd hours of the day and night, and wrote so eloquently about that experience. Admittedly, this is not easy to do in the modern era, and I am grateful for the role models who showed me how an ideal home visit is done.
Usually, after all the treatments—surgery, chemotherapy, radiation and experimental therapy—are done, and there is still suffering despite control of pain and symptoms, I have offered to see patients at home. I make an appointment and arrive without a white coat, without equipment and without a black bag. I have learned that my presence matters; empathy and compassion matter. We address concerns at the bedside, sometimes at the kitchen table, and often on the porch or driveway. I have seen how silence is not stressful. Minutes go by without conversation, but comfort is offered. I don’t feel alone; hospice teams are on the front lines and work with me.
Broadway and Ridgecrest, San Antonio: Jackie always spoke about La Crema, her favorite pinot noir, especially on days that were a struggle. “Look what they did to my boobs!” she said. She was feisty. Her mother, a retired oncology nurse, looked on as only a mother who had decades of breast oncology under her belt can look at her offspring. Jackie had brought her dachshund to the breast cancer clinic on her last Christmas, with the dog in a Santa outfit with the red hat strapped on. Now she lay in her apartment. Through the haze of morphine, she beckoned her mom close. “Give Dr. Karnad the third bottle from the left on the top row. That’s a Lodi zin; and then, here, take the last one on the bottom row. That’s a buttery chardonnay. I won’t be drinking them. Might as well give them away!”
Guilbeau Road, San Antonio: A young couple from India. He was stoic, tall, mostly silent. The cancer had jumped from his parotid gland under his right ear and was now strangling his small and large bowel in half a dozen places. She spoke for him. He wanted no surgery, no treatment. It took nearly a year to bring him to his deathbed. By then he had somehow managed to maneuver soft rice through the dead ends of his obstructed bowel; how, I never knew. Parents from Kerala had arrived. His mother told me softly, “He doesn’t even like my tea.” The next time I saw him was at the Morningside Inpatient Hospice Unit. Wailing family packed the halls, and I leaned in to offer my condolences.
Even as a revolution in science brings new treatments for cancer nearly every day, there is a need to focus on the control of pain and suffering as we seek new ways to prevent and treat this disease. There is a saying that many caregivers live by: “To cure sometimes, to relieve often, to comfort always.” Being able to see a patient at home may be a huge comfort to those in that home. And in so many ways, it’s a comfort to me as well.

Talking it out
By Joel Williams
Talk therapy can lead to recovery from post-traumatic stress disorder for those who suffer from combat-related PTSD. This was the finding in the largest clinical trial to date documenting an evidence-based treatment for active-duty military personnel.
Cognitive processing therapy, a leading talk therapy used for civilians with PTSD, was found effective for nearly half of those receiving 12 sessions of the therapy in individual format over the course of six weeks. Nearly 40 percent of those receiving group therapy recovered from PTSD. The findings, published online in JAMA Psychiatry, showed significant reductions in PTSD symptoms, as well as a decrease in depression and suicidal thinking, all of which were maintained for six months.
The trial was conducted at the U.S. Army’s Fort Hood in Killeen, Texas, for the multi-institutional STRONG STAR Consortium, which is funded by the U.S. Department of Defense and based at UT Health San Antonio.
Patricia Resick, Ph.D., the developer of cognitive processing therapy and professor of psychiatry and behavioral sciences at Duke University School of Medicine, led the study comparing the two different ways of delivering the treatment. The therapy helps patients challenge distorted thoughts that perpetuate unhelpful emotions related to their trauma, such as guilt, blame and anger, and to process their natural emotions, leading to a healthier viewpoint and more control over traumatic memories.
In the clinical trial, 268 active service members diagnosed with combat-related PTSD were assigned randomly to receive cognitive processing therapy either in individual or group format. The research team found both formats were effective for many patients, but those receiving individual therapy showed significantly greater improvement.
“This is very encouraging, especially since the trial was based only on 12 sessions of therapy over six weeks,” said Dr. Resick, the paper’s first author. “People often think you have to go to therapy for years to address PTSD. But in this large-scale clinical trial, we saw such a large percentage of patients show significant improvements and even fully recover from PTSD in a matter of weeks. This makes the therapy a good option for service members who wish to stay fit for active duty and veterans seeking to reintegrate into civilian life.”
While concluding that individual cognitive processing therapy is the more effective means of delivering treatment, the research team also suggested that group therapy should remain an option when there is a shortage of available therapists.
“The results of this study provide the strongest scientific evidence to date that combat-related PTSD can be effectively treated in active-duty military personnel,” said co-author Alan Peterson, Ph.D., director of the STRONG STAR Consortium and professor in the Department of Psychiatry at UT Health San Antonio. However, he added, there still is room for improvement in order to help more service members heal from their psychological wounds.
This trial with veterans is the latest that shows added difficulty in treating combat-related PTSD as compared to PTSD in civilians.
“In the military population, much remains to be done to improve existing treatments like [cognitive processing therapy] or develop new treatments,” the researchers concluded.
They suggested additional research should focus on specific issues found in military populations that may affect PTSD treatment, including a look at the roles of substance abuse and traumatic brain injury, and assessing the potential benefits of varying treatment length according to patient needs.
“Already, the STRONG STAR Consortium is starting to address many of these issues, with additional clinical trials in progress that seek to tailor and enhance [cognitive processing therapy] for combat-related PTSD and improve its effectiveness with service members and veterans,” Dr. Peterson said.

Appointments
 Tim Huang, Ph.D., was named interim director of the UT Health Cancer Center, formerly referred to as the Cancer Therapy & Research Center. He has served as deputy director of the center and as chair and professor of molecular medicine. He holds the Alice P. McDermott Distinguished University Chair.
Tim Huang, Ph.D., was named interim director of the UT Health Cancer Center, formerly referred to as the Cancer Therapy & Research Center. He has served as deputy director of the center and as chair and professor of molecular medicine. He holds the Alice P. McDermott Distinguished University Chair.

M. Danet Lapiz-Bluhm, Ph.D., RN, associate professor in the School of Nursing, has been named a collaborative academic research member of the Veterans’ Action League. The multistate project will empower veterans to have an active voice in how veteran health care is delivered in the future.
 Randal Otto, M.D., was appointed director for clinical affairs and physician-in-chief of the UT Health Cancer Center. He has served as associate dean of special programs in the Joe R. & Teresa Lozano Long School of Medicine, and holds the Thomas Walthall Folbre, M.D., Endowed Chair in Otolaryngology.
Randal Otto, M.D., was appointed director for clinical affairs and physician-in-chief of the UT Health Cancer Center. He has served as associate dean of special programs in the Joe R. & Teresa Lozano Long School of Medicine, and holds the Thomas Walthall Folbre, M.D., Endowed Chair in Otolaryngology.
 Ronald Rodriguez, M.D., Ph.D., was appointed as interim dean of the Long School of Medicine. He joined UT Health San Antonio in 2013 as the Henry B. and Edna Smith Dielmann Memorial Professor of Urologic Science, and has served as the chairman of the Department of Urology.
Ronald Rodriguez, M.D., Ph.D., was appointed as interim dean of the Long School of Medicine. He joined UT Health San Antonio in 2013 as the Henry B. and Edna Smith Dielmann Memorial Professor of Urologic Science, and has served as the chairman of the Department of Urology.

Awards
 Ralph DeFronzo, M.D., professor of medicine and chief of diabetes in the Joe R. & Teresa Lozano Long School of Medicine, has been selected to receive the 2017 Harold Hamm International Prize for Biomedical Research in Diabetes, which includes $250,000.
Ralph DeFronzo, M.D., professor of medicine and chief of diabetes in the Joe R. & Teresa Lozano Long School of Medicine, has been selected to receive the 2017 Harold Hamm International Prize for Biomedical Research in Diabetes, which includes $250,000.

Bess Frost, Ph.D., assistant professor of cell systems and anatomy at the Barshop Institute for Longevity and Aging Studies, has been awarded the 2016 New Investigator Award in Alzheimer’s Disease from the American Federation for Aging Research.
 Robin Jean Leach, Ph.D., professor of cell systems and anatomy and chief of the Division of Research in the Department of Urology, was named a Piper Professor by the Minnie Stevens Piper Foundation.
Robin Jean Leach, Ph.D., professor of cell systems and anatomy and chief of the Division of Research in the Department of Urology, was named a Piper Professor by the Minnie Stevens Piper Foundation.
 Amelie G. Ramirez, Dr.P.H., professor of epidemiology and biostatistics and director of the Institute for Health Promotion Research, received the American Association for Cancer Research Distinguished Lecture on the Science of Cancer Health Disparities award.
Amelie G. Ramirez, Dr.P.H., professor of epidemiology and biostatistics and director of the Institute for Health Promotion Research, received the American Association for Cancer Research Distinguished Lecture on the Science of Cancer Health Disparities award.
 John Rugh, Ph.D., professor of developmental dentistry, received the Evidence-Based Dentistry Faculty Award from the American Dental Association and the American Association of Dental Research.
John Rugh, Ph.D., professor of developmental dentistry, received the Evidence-Based Dentistry Faculty Award from the American Dental Association and the American Association of Dental Research.

Now open
 When UT Health Hill Country opened in February in Boerne, it was “no small feat” to stray from the traditional model of an academic health center located in the heart of an urban setting, said UT Health San Antonio President William L. Henrich, M.D., MACP.
When UT Health Hill Country opened in February in Boerne, it was “no small feat” to stray from the traditional model of an academic health center located in the heart of an urban setting, said UT Health San Antonio President William L. Henrich, M.D., MACP.
The 19,000-square-foot facility brings a comprehensive array of services, including primary care, orthopaedics, radiology, physical therapy, urology, behavioral health and lab services to the high-growth area northwest of San Antonio.
“We hope this is just the beginning,” Dr. Henrich said. “We hope to [open centers] more and more around the city.”
Carlos A. Rosende, M.D., executive director of UT Health Physicians, said a unique aspect of the clinic is that it is linked to the more than 700 physicians in 120 specialties in the overall UT Health physician practice. It also expands teaching venues for students and trainees and enhances clinical research of the Joe R. & Teresa Lozano Long School of Medicine.
In 2015, the UT System Board of Regents approved $19.5 million for construction, equipment and land acquisition. The facility includes exam rooms, conference rooms, physician offices, waiting rooms and a full-service imaging center with magnetic resonance imaging (MRI), CT scan technology and X-ray areas.
UT Health Hill Country is located at 25723 Old Fredericksburg Road in Boerne, a quarter of a mile from Ralph Fair Road.
Colliding, bumping, smashing
They’re in every cell in every living organism, and now researchers have a better understanding about heat shock proteins, also called chaperone proteins, and their role in human diseases.
The proteins were first identified in cells subjected to heat. They help the body maintain proper protein function and, importantly, prevent the accumulation of damaged proteins. This accumulation is thought to be important in the development of diseases of the brain such as Alzheimer’s and Parkinson’s.
Heat shock proteins with a molecular weight of 70 can break apart protein complexes rather than simply binding to them. Called Hsp70s, they collide with them and generate a force that dissolves the complexes.
“No one knew how the heat shock proteins pull apart bad protein complexes,” said Rui Sousa, Ph.D., a professor of biochemistry in the School of Medicine who authored a study with biochemistry professor Eileen M. Lafer, Ph.D., in the journal Nature Structural & Molecular Biology.
“At the molecular level, everything is moving, colliding and bumping, and smashing into other components of the cells. We found that the system moves Hsp70s to where they are needed. Once this occurs, collision pressures pull things apart.”
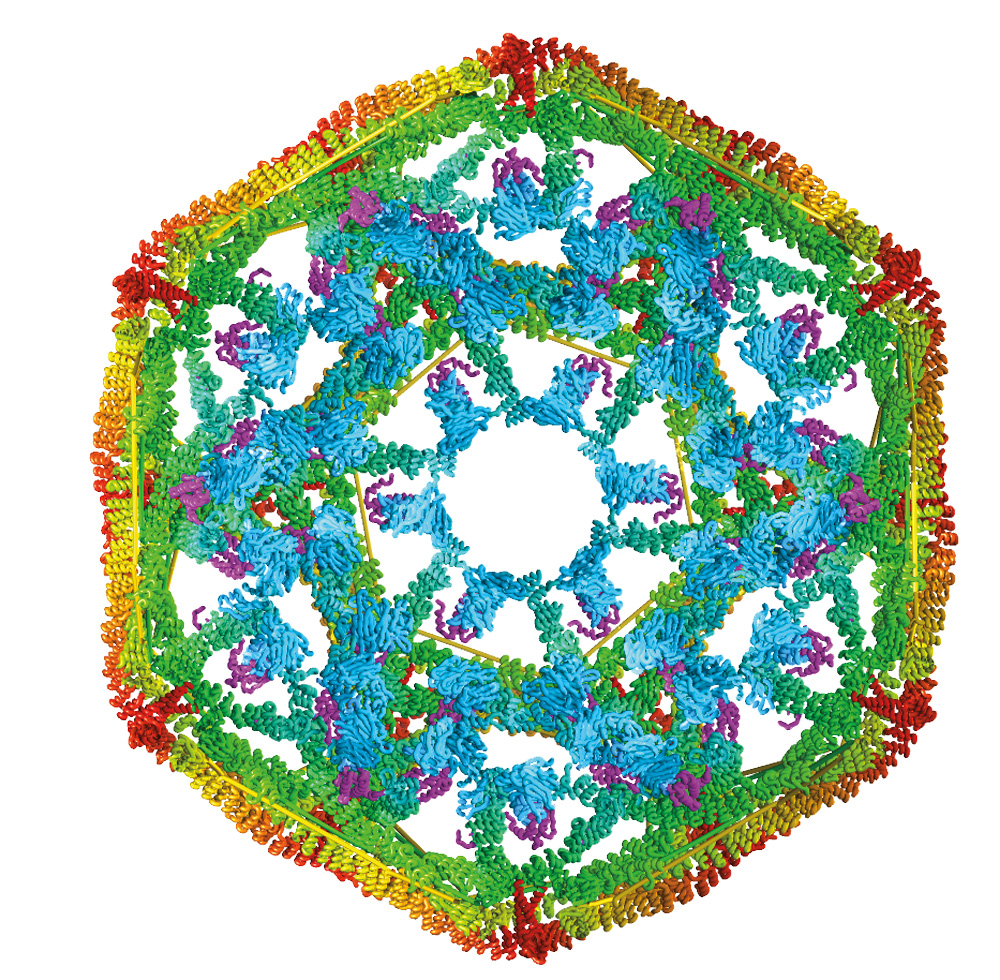
They studied clathrin, a protein that is uniform in size and shape and is important in making intracellular cages that transport other proteins.
Dr. Lafer grew clathrin “cages”—shaped like microscopic soccer balls—that provided the biological raw material for Dr. Sousa and the team to study the force that occurs with Hsp70 collisions. The clathrin model system could be manipulated to yield precise results.
By making variants of clathrin with recombinant DNA technology, team members were able to manipulate this biological material in ways that allowed them to determine the mechanism by which it is taken apart by Hsp70.
“This work was a tour de force, requiring the convergence of exceptional biochemical and molecular genetic skills with a deep understanding of the principles of physical chemistry,” said Bruce Nicholson, Ph.D., chair of the Department of Biochemistry. “Such insights into the most basic aspects of protein chemistry and cell biology are often, as in this case, driven by a curiosity to find out how the molecular machines that drive our bodies work. But from these basic pursuits of scientific curiosity will often stem great benefits to human health.”
Understanding Hsp70 behavior may have relevance to human disease. By increasing Hsp70 function, scientists cured Huntington’s, a neurodegenerative disease, in a fly model. Tumors rely on Hsp70s to survive, so lowering Hsp70 function also is a topic in cancer research.

Miles of smiles
If one child’s smile can warm the heart, imagine what tens of thousands can do.
That’s the reality in Laredo, where Miles of Smiles–Laredo has brought free dental care to elementary school children since 2006.
Miles of Smiles–Laredo is a School of Dentistry public health program directed by David P. Cappelli, Ph.D., D.M.D., M.P.H., professor and director of the research division in the Department of Comprehensive Dentistry.
The program’s reach has expanded from two schools to 47 schools in a decade. That’s about 10,000 children each year who receive free care.
Using portable dental equipment, a team of one dentist and three dental assistants from UT Health’s Laredo campus spend two to four days in each school, providing dental screenings, fluoride varnish and dental sealants.
It’s estimated that over $470,000 in uncompensated dental services were provided in Webb County last year.

Breaking down the prison walls
Individuals with post-traumatic stress disorder relive past traumas again and again, bound in a virtual prison of their memories.
Researchers in the School of Medicine now report a biological mechanism that might explain why these individuals are less able to extinguish the fear of past dangers.
The new research centers on the hormone adiponectin, which is secreted by fat cells called adipocytes. The scientists studied a mouse model of PTSD.
These mice were trained to associate a setting, such as a box, with a mild unpleasant stimulus. As expected, they showed a fear response when re-exposed to the setting.
Mice deficient for adiponectin and its receptor formed fearful memories just like healthy mice, but when placed again in the same setting minus the unpleasant stimulus, were slower to let go of the fear.
Injecting adiponectin prior to this training prompted faster learning to overcome fear, the measurements showed.
“Once the threat is no longer there, the fear should go away, but in PTSD it keeps flashing back,” said study senior author Xin-Yun Lu, M.D., Ph.D., professor of pharmacology and a member of the Barshop Institute for Aging and Longevity Studies. “In the PTSD animal model, the circulating adiponectin is low, data suggest. If the genes encoding adiponectin and its receptor are disrupted, the mice extinguish fear responses much slower. If adiponectin levels are elevated in the brain, the mice get extinction faster.”
Adiponectin impairment is implicated in metabolic diseases such as obesity and type 2 diabetes. The new research, published in the journal Molecular Psychiatry, shows the hormone has a role beyond its metabolic control, Dr. Lu said.
“To date, medication treatments for PTSD have been of limited benefit,” said Alan L. Peterson, Ph.D., ABPP, professor of psychiatry and director of the STRONG STAR Consortium and the Consortium to Alleviate PTSD. “Dr. Xin-Yun Lu’s work holds significant promise for the development of new, more effective medication treatments for PTSD.”
UT Health San Antonio has filed for patent protection on the finding because it may eventually lead to a drug to treat PTSD, which affects an estimated 8 percent of the civilian population and up to 15 percent of U.S. active-duty and retired service personnel.

New entry-point
The School of Health Professions is offering one of the country’s few entry-level master’s degree programs in medical laboratory science. It’s an opportunity for those looking to enter San Antonio’s $30.6 billion biomedical and health care industry, officials said.
Medical laboratory scientists are a critical part of the health care team who analyze medical samples in the clinical laboratory, and the job outlook is excellent, said Cheryl Burns, M.S., associate professor and director of the master’s degree program in laboratory science.
“We make a significant difference in the quality of patient care. Physicians rely on laboratory test results in diagnosing illnesses and monitoring how patients are progressing in their treatment,” she said.
Nearly 100 percent of graduates of the clinical laboratory sciences program are offered jobs after graduation.
While the 24-month bachelor’s degree in clinical laboratory sciences will continue to be offered, the new 27-month master’s program is designed to provide deeper knowledge to students who already have a bachelor’s degree in another field. It is expected to prepare students for higher-level positions and better potential for advancement, Burns said.