
Warriors for health
They were medical specialists and transport pilots in some of the world’s most hostile regions. They defended the nation in the cyber realm, and faced their own mortality multiple times a day as explosions erupted around them.
Today their service is of a different kind. They are in hospital rooms and clinics, classrooms and research labs. They are among the hundreds of students who seek careers in health professions after years of military service. They are the 64 students currently attending classes at the Health Science Center while on active-duty military scholarships, and the 433 faculty and staff members who also carry the distinction of being military veterans.
“We are fortunate to have many heroes at the Health Science Center. They bring a maturity and unique perspective to their work, having served in developing nations and combat environments,” said retired Air Force Maj. Gen. Byron C. Hepburn, M.D., director of the Military Health Institute, created in 2014 to strengthen partnerships with the military. Dr. Hepburn’s own military career spanned 38 years.
“What we are doing here at the Health Science Center is worthy work and in true service to our fellow man. There’s no greater professional satisfaction than that. No matter what we’re doing at the university, we’re all contributing to that mission.”
Here are some of their stories.
 Rudy Gomez suspects it was a high-powered assault rifle that fired the shots. He was in Habbaniyah, Iraq, serving as a Navy corpsman, an enlisted medical specialist attached to a U.S. Marines infantry unit.
Rudy Gomez suspects it was a high-powered assault rifle that fired the shots. He was in Habbaniyah, Iraq, serving as a Navy corpsman, an enlisted medical specialist attached to a U.S. Marines infantry unit.
“The round went completely through my thigh, severed my sciatic nerve and partially affected nerves in my calf,” he said. “It paralyzed part of the calf and I lost about 90 percent of the mobility in my foot.”
The year was 2008, and after six years in the Navy, Gomez was medically discharged at Camp Lejeune, N.C.
“While I was being discharged, I was surrounded by military medical personnel, many of whom were giving me career options,” he said. “I knew then that I wanted to become a physician assistant.”
During his service in Iraq, Gomez went on Humvee and foot patrols with Marines doing security checks. Their health and welfare was largely his responsibility—as the unit’s medic, he was the one who would work to keep the Marines alive if casualties occurred.
“I worked as their doc. They call you doctor and they expect you to know everything,” he said. “They expected a lot because I was the only medical guy out there with them.”
His own injury gave him even greater perspective on the role of a health care provider.
“Prior to my service in the military, I did not have the patient perspective,” he said. “In my early service, I assisted those who helped patients. But when I was injured, I saw up close and personal that all providers are different. Some are incredible and outstanding, and unfortunately some are not.
“I got the chance to learn what kind of provider I want to be—the kind who builds trusting relationships with patients.”
 For Robert De Lorenzo, M.D., working in the leading combat support hospital during the war in Iraq was a lot like living through episodes of M*A*S*H.
For Robert De Lorenzo, M.D., working in the leading combat support hospital during the war in Iraq was a lot like living through episodes of M*A*S*H.
Working 12-hour shifts usually seven days a week, Dr. De Lorenzo and his colleagues went through calm times when soldiers and civilians weren’t getting hurt, but then frenetic times when the workload surged.
“If you watch old reruns of M*A*S*H, there were boring times in their tents and other times when casualties kept coming into the hospital. That’s not far from the truth,” he said.
Dr. De Lorenzo, professor and research director of the Department of Emergency Medicine, joined the Army in 1994. He followed his father, grandfather and uncles who had all completed stints in the service. He served tours of duty in Iraq in 2005-06, and 2010, and was assigned to the 10th Combat Support Hospital in Baghdad, the busiest trauma center in the world at the time.
“While it was professionally rewarding to lead a team and use the skills of a physician to try and save lives, it was an incredibly sobering experience at the same time,” he said. “Day in and day out we saw shattered young bodies. Many were U.S. soldiers, but of course others were Iraqi soldiers and citizens, even children.”
Veterans, particularly those who have seen combat, provide a unique perspective on the world and clinical care that is particularly useful for a medical student, he said.
“As medical providers, both international law and the mores and ethics of medicine demand that we give the same care to everyone,” he said. “The military medical veterans are proud of having accomplished that.”
Dr. De Lorenzo’s research interest is shaped
by his wartime experience. While in Iraq, he treated numerous trauma patients with injuries to their airways.
“The airway remains an important gap area in care,” he said. “There haven’t been many significant innovations or advances in airway management, and our soldiers and the public need better tools in that area.”
 Members of the Navy’s Sea, Air and Land teams—better known as SEALs—are almost mythical beings. They are able to thrive in situations where others could barely function. They are the group the U.S. military calls in when the margin for error is nonexistent.
Members of the Navy’s Sea, Air and Land teams—better known as SEALs—are almost mythical beings. They are able to thrive in situations where others could barely function. They are the group the U.S. military calls in when the margin for error is nonexistent.
So it is perhaps no surprise that the final leg of their training has become popularly known as “Hell Week.”
“You’re wet and awake for an entire week,” explained Nicolas Walsh, M.D. “You’re basically always in frigid water, and asked to perform at peak levels without fail. Almost everyone who is going to quit, drops out that week.”
By the end of Hell Week, almost 75 percent of each class of candidates has withdrawn.
“We started with 217 individuals, all fully able to complete this training,” Dr. Walsh recalled. “Only 56 finished.”
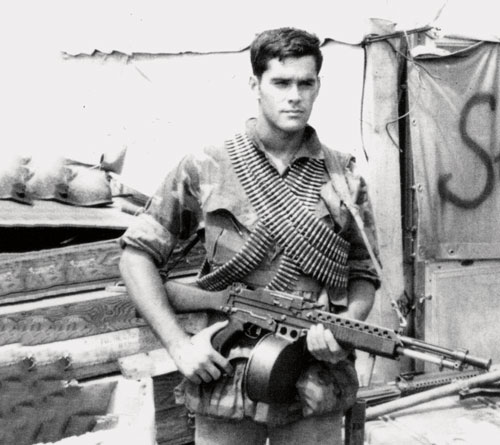
Dr. Walsh was one of the 56. He served two tours in Vietnam, from 1970 to 1972, as a part of SEAL Team One, and became highly decorated for his service. Dr. Walsh earned two Silver Stars for heroism and a pair of Bronze Stars—among many other commendations.
Navy SEALs in Vietnam packed light, carrying only ammunition and essential weaponry as they became ghosts, working as strike forces to gather—and act upon—intelligence.
Out of necessity, SEALs learn to critically analyze and decisively respond to ever-changing environments and situations. This requires one to think outside the box and adapt, before taking appropriate action.
That training has served Dr. Walsh well throughout his career as professor and chairman of the Department of Rehabilitation Medicine for 26 years.
“SEAL training is one of the hardest challenges one can face both physically and mentally,” Dr. Walsh said. “But not everyone is a SEAL. So the experience is, essentially, no different than one faced by somebody else going through the most difficult trial of their own life. It’s very easy for me to have a great deal of empathy for our patients, whether they’re enduring a spinal cord injury, traumatic brain injury, a stroke or any other kind of physical challenge. Fortunately, we’re able to help a great many people.”
 Roger Weed, D.D.S., FACD, flew about 1,000 injured soldiers to safety during the Vietnam War as a dustoff pilot, but on one jungle landing, bullets flying through his helicopter turned him into the patient.
Roger Weed, D.D.S., FACD, flew about 1,000 injured soldiers to safety during the Vietnam War as a dustoff pilot, but on one jungle landing, bullets flying through his helicopter turned him into the patient.
“We were going into an area where we always got shot at—a very hostile area close to North Vietnam,” said Dr. Weed, now an associate professor of comprehensive dentistry. “Politically, it was a remote part of the country. The shooters probably didn’t know who we were. They just knew they didn’t want us there.”
The chopper landed, and the patient was loaded for transport. Then the shooting began.
“Probably 30 rounds went into the back of the helicopter and the back of my seat and me,” Dr. Weed recalled. “Nobody else was hit and when I looked at the sleeve of my fatigues, there were bullet holes in it. I couldn’t move my left arm.”
The radial nerve that controls the triceps was severed.
“Army medicine put it back together,” Dr. Weed said. “In 1967, microsurgery was rare but a neurosurgeon at Brooke Army Medical Center did the microsurgical reattachment.”
It took three surgeries and about a year of therapy for him to return to the field.
By 1968, he was again overseas, this time in Korea, where the spy ship U.S.S. Pueblo had been captured by the North Koreans. Now a captain, he assisted with returning the officers and crew to the U.S.
Dr. Weed left active duty in 1969 to attend dental school, but served in the Army Reserves for 34 more years, retiring as a dental corps colonel in 2003.
“Overall, I’ve been able to do two careers at once, both dentistry and the military,” he said.
Dr. Weed’s military experiences strongly shape his approach to dentistry.
“Just as a pilot must have a mission, an objective and route to get there, a dentist must also be well organized and have plans for how things are supposed to be done,” he said. “My flight training has probably been as beneficial as anything.”
 Cherita Johnson didn’t think she’d ever want to be a nurse. From her mother’s own experience in the field, she knew it was a difficult job. But while serving in the Air Force, she had a chance to experience nursing firsthand, and it changed her life.
Cherita Johnson didn’t think she’d ever want to be a nurse. From her mother’s own experience in the field, she knew it was a difficult job. But while serving in the Air Force, she had a chance to experience nursing firsthand, and it changed her life.
“In Afghanistan, I was able to assist with a few things during an attack, and that memory became my driver to get my degree in nursing,” she said.
Johnson, an active-duty servicewoman and undergraduate student, has protected network security at U.S. Air Force installations from South Korea to Afghanistan to Germany for most of her 17 years of service.
But whenever she could, she volunteered in hospitals and found her true passion.
“Caring for someone who can’t necessarily care for themselves, and being a voice for someone who can’t speak for themselves, advocating for the best possible care for them, was rewarding,” she said.
After completing her nursing degree in May, Johnson would like to work in flight or medical evacuation nursing for the Air Force and reach 25 years of service. After she retires from the military, she’d like to open a palliative hospice care management service.
“I enjoy the intensity of what I believe those areas of nursing will bring,” she said. “I think I work well under pressure, and I bring leadership and management skills from my years in the military.
“I am proud to serve every day, and proud that I can protect people’s families.”
 Mara O’Sullivan grew up hearing stories of children playing around landmines—a harsh contrast to her own cheerful sandbox. Her father, an Army officer, and her mother were certified nurse anesthetists and moved their family around the world.
Mara O’Sullivan grew up hearing stories of children playing around landmines—a harsh contrast to her own cheerful sandbox. Her father, an Army officer, and her mother were certified nurse anesthetists and moved their family around the world.
“My father came back with stories such as surgery on a person who had stepped on a landmine in Kosovo,” O’Sullivan said. “At 8 or 9 years of age, I was thinking about global engagements, knowing things other children never consider.”
Her parents instilled in her the ethical responsibility of health care providers to serve all of humanity, regardless of dividing lines. O’Sullivan, a 2014 graduate of the U.S. Air Force Academy, will serve a minimum of nine years after graduating medical school in 2018 and completing her residency.
“The reason I decided to become a military doctor is you get a chance to serve people in combat, and also their families,” she said.
She also seeks exposure to the broadest range of military medical experiences, from running a clinic or hospital at a new duty station to setting up a temporary hospital while on deployment.
“When you deploy for military medicine especially, you treat anybody who comes through your doors,” she said. “If they’re locals, insurgents or children who just happen to be nearby, you treat them as you treat our own.
“We use the same resources on everybody regardless of nationality or sides of the political war. Your service is to be a doctor and an officer, but you don’t need to hold a gun to do that. I don’t need to compromise my ethics to do that.”
 Jeff Marrs learned the value of restraint while serving as commander of a U.S. Army “breach” platoon in Anbar province, Iraq. While clearing a path to a suspected terrorist camp, Marrs faced a decision of whether to blow up a wall that blocked entry to a village.
Jeff Marrs learned the value of restraint while serving as commander of a U.S. Army “breach” platoon in Anbar province, Iraq. While clearing a path to a suspected terrorist camp, Marrs faced a decision of whether to blow up a wall that blocked entry to a village.
They hadn’t encountered enemy fire. He decided not to use explosives.
“We went around the wall, still not receiving any enemy contact,” he said. “On the other side, at the site where we were going to detonate, was a room full of women and children. For me it was a consideration of restraint. I consider that to be a very smart decision.”
Marrs was 24 when he assumed command of his first platoon in April 2003. Operating out of an Army base in Mosul, Iraq, the platoon provided support and stability to local nationals. This included patrols to counter attacks by improvised explosive devices.
“I vividly remember three or four enemy attacks,” Marrs said. “Thankfully we didn’t take any wounded or killed.”
The platoon also worked to bolster the economy. Marrs was asked to run a propane facility in northern Iraq. The platoon coordinated with the locals to increase production—important because propane is the primary source of cooking for the people.
In 2004 he returned to the U.S., but deployed again to Iraq in September 2005 as a battle captain, coordinating emergency responses 10-14 hours a day for 10 months. Each day brought six to eight enemy attacks.
He left active duty in 2008 and entered the Texas National Guard. Two years later, he was sent to Afghanistan. It was this deployment that changed the course of his career.
“I made the decision to become a dentist on my third deployment,” Marrs said. “I met a deployed dentist, Jeff Aycock, who was assigned to Hamid Karzai International Airport in Kabul. He said, ‘You have great teeth, you’re a West Point graduate, you’ve been to Ranger School, you’ve had multiple years of experience, you should be a military dentist.’ I kind of laughed it off, but saw him treating all the multinational soldiers, and that encouraged me to consider it.”
Marrs entered the School of Dentistry in 2013. His scholarship requires him to return to active duty after graduation.
“When I graduate in 2017, I will return to the military as a dentist and pursue an orthodontics residency, and then hopefully continue to provide excellent care to our soldiers, spouses and their children,” he said.
“As I’ve done throughout my career, I will try to be at the point where I can provide the most benefit to the largest amount of people.”
In November 2006, Ryan P. Gilley was a combat engineer who had spent almost a year in Baghdad clearing roadside bombs while trying to reconcile the dissonance between war and the smiles of Iraqi children delighted with the soccer balls he and other soldiers gave them.
After three years of active duty, Gilley yearned for civilian life. In January 2007, within two months of returning from Iraq, Gilley was sitting in college classrooms, immersed in science.
“I like to solve puzzles and fix things, and so I think inherent in that is kind of an enjoyment of things that are somewhat mysterious,” he said. “You know there are these microbes all over but we can’t see them. You can’t see the bacteria and the viruses. You have to have equipment that helps you find them.”
Gilley began doctoral studies in microbiology and immunology in 2012 and in April defended his dissertation. He will begin a post-doctoral fellowship this summer on the effect of streptococcus pneumoniae on the heart and how the heart cells die in response to the bacteria. Researchers found the bacteria can create holes in the cardiac tissue of mice.
“My dissertation has been based on further characterizing what happens and what the bacteria require, the protein requirements that the bacteria need in order to get into the heart to cause these little lesions,” he said.
As he works toward his goal of a faculty position and a lab of his own, Gilley said his time in the military seems both distant and fresh.
“I don’t regret at all my time in the Army,” he said. “I had a good time and there were bad times. That was not the life I wanted to have but I don’t regret doing it.”

Conquering a parasitic demon
The emaciated girl’s stare. The lethargic boy’s protruding belly. The inert mother. From the sands of Egypt and Morocco to the rainforests of Brazil and Southeast Asia, Phil LoVerde, Ph.D., professor of biochemistry and pathology in the School of Medicine, has observed the human toll of schistosomiasis, the world’s most common parasitic disease after malaria.
In oases and villages, he has been a welcome visitor—a scientist sifting through clues like a detective, ever on a mission to end the menace and relieve the suffering.
“I’ve worked on ‘schisto’ my whole life,” Dr. LoVerde said. Indeed, searching for a better treatment has been his life’s work, and with the help of colleagues at Texas Biomedical Research Institute and The University of Texas at San Antonio, Dr. LoVerde is developing a new therapy to control the spread of schistosomiasis worldwide. A $3 million, five-year grant to the Health Science Center from the National Institute of Allergy & Infectious Diseases funds the studies.
Schistosomiasis, also called snail fever, is an infection of the larval worms of freshwater snails. These larvae, the size of a fleck of dust, infect 261 million people in 78 countries, according to the World Health Organization. Two-thirds of the world’s cases are in Africa.
[bgsection pex_attr_title="" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="" pex_attr_image="" pex_attr_imageopacity="1" pex_attr_bgimagestyle="static" pex_attr_titlecolor="ffffff" pex_attr_textcolor="a8230c" pex_attr_height="500"]
Like mosquitoes transmit malaria, freshwater snails carry deadly larval worms that infect millions of people worldwide.
Source: World Health Organization
[/bgsection]
Infections result from contact with infested water during activities such as fishing, swimming and washing clothes.
“I’ve seen people who frequent the contaminated waters every day of their lives and are constantly exposed to the parasite,” Dr. LoVerde said.
Infections usually affect the urinary tract, liver and intestines, causing symptoms such as blood in the urine. While the disease doesn’t kill most victims, it is a chronic drain, causing subtle effects such as underperformance in schoolchildren who are anemic from blood loss. Children are stunted in their growth patterns if they have a heavy infection, Dr. LoVerde said, and their reproductive development is slower than that of uninfected children.
“It has a major impact on their future, there’s no question,” Dr. LoVerde said.
Dr. LoVerde began working in Egypt in 1970 and lived there for a year with his family, doing fieldwork on the Upper Nile near Aswan and Luxor. He also spent extensive time in Brazil.
“In the early days we searched for snails, but later we did genetic studies to learn the role people’s genes play in infection outcomes,” he said. “In Brazil we went house to house with an interpreter speaking Portuguese, asking, ‘who’s your mother, who’s your father, who’s your brother or sister, who’s your uncle, who’s your cousin?’ We used this information to establish a pedigree, and from it we found that, about 40 percent of the time, a person’s genes play a key role in infection outcomes.”
The genetic detective work also included analysis of the worms’ own genes, particularly the ones that allow the parasite to develop drug resistance. The most frequently prescribed medication, praziquantel, is plentiful and inexpensive, but as its use increases, the parasite’s resistance increases.
“Several funders are donating 250 million pills of praziquantel per year for each of the next five years to prevent the infection in Africa,” Dr. LoVerde said. “If the parasite develops drug resistance, the concern is we won’t have a backup. We need a drug that can be used in combination with praziquantel.”
The scientists are turning to a 40-year-old drug called oxamniquine for a solution. But improvements need to be made, they said. While praziquantel kills three schistosome species, oxamniquine in its original form killed only one, and that one species has been known to develop drug resistance.
In 2009, Dr. LoVerde was part of a team that published the sequence of the schistosome genome in Nature. In collaboration with geneticist Tim Anderson, Ph.D., of Texas Biomedical Research Institute, they used this information to develop a genetic map. This allowed the scientists to identify the gene responsible for drug resistance in the worms.
By 2013, working with P. John Hart, Ph.D., professor of biochemistry and director of the X-ray Crystallography Core Laboratory at the Health Science Center, the researchers determined the crystal structure of the gene’s protein—a discovery published in Science.
“We showed the details of how oxamniquine binds to this protein and how the drug works,” Dr. Hart said.
Armed with this information, the researchers turned to UTSA’s medicinal chemist Stanton McHardy, Ph.D., part of the Center for Innovative Drug Discovery, a joint initiative of the Health Science Center and UTSA. Dr. McHardy and students are taking the crystal information and making new derivatives—new modified compounds—of oxamniquine.
“Stan has made more than 80 compounds based on the information we have provided,” Dr. LoVerde said.
Two derivatives kill between 40 and 80 percent of two different schistosoma species, they found.
“It’s amazing,” Dr. LoVerde said. “What we are doing works.”
Dr. LoVerde recently traveled again to an isolated area of Brazil, where he collected samples of worms. The team found five different mutations that lead to drug resistance to oxamniquine. The team will assess ways to block the problem.
“This shows the power of genetics and molecular biology to understand and address a disease,” Dr. LoVerde said.
By understanding why the parasite becomes resistant, the team may soon have a viable option to fight the spread of schistosomiasis, and help the 261 million infected people and the half-billion more who are at risk around the world.
[bgsection pex_attr_title="Essay: Under attack" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-dark-bg" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="000000" pex_attr_textcolor="000000" pex_attr_height=""]By Gregory M. Anstead, M.D., Ph.D.
 In 2011, I participated in a medical mission trip to Senegal with a group from University United Methodist Church from San Antonio. In one particular village near the city of M’bour, we encountered many cases of urinary schistosomiasis, due to the parasitic flatworm Schistosoma haemotobium. In the dry season, this region of Senegal is a parched and dusty place. This village was lucky enough to have a nearby lake, which provided water for drinking and cooking, irrigation, and for raising livestock. But lurking in the water was a microscopic fork-tailed demon, the larva of the schistosoma flatworm. As the villagers gathered water from the lake, they were attacked by these larvae. The larvae burrowed into the skin of their unsuspecting victims, entered their blood stream and travelled to the liver to mature into adult flukes (flatworms). After about three weeks or so, flukes migrate to the veins of the urinary bladder to mate. The female fluke lays hundreds of eggs per day, which migrate to the urinary bladder and ureters and are excreted in the urine. If the egg-laden urine enters a water source, the life cycle of this parasite starts again.
In 2011, I participated in a medical mission trip to Senegal with a group from University United Methodist Church from San Antonio. In one particular village near the city of M’bour, we encountered many cases of urinary schistosomiasis, due to the parasitic flatworm Schistosoma haemotobium. In the dry season, this region of Senegal is a parched and dusty place. This village was lucky enough to have a nearby lake, which provided water for drinking and cooking, irrigation, and for raising livestock. But lurking in the water was a microscopic fork-tailed demon, the larva of the schistosoma flatworm. As the villagers gathered water from the lake, they were attacked by these larvae. The larvae burrowed into the skin of their unsuspecting victims, entered their blood stream and travelled to the liver to mature into adult flukes (flatworms). After about three weeks or so, flukes migrate to the veins of the urinary bladder to mate. The female fluke lays hundreds of eggs per day, which migrate to the urinary bladder and ureters and are excreted in the urine. If the egg-laden urine enters a water source, the life cycle of this parasite starts again.
In the ureters and urinary bladder, the eggs elicit an inflammatory response that leads to hematuria (blood in the urine), and blockage of the ureters, which can lead to urinary tract infections, and damage to the kidneys. With time, this prolonged inflammation can lead to bladder cancer.
In this village, we collected samples of urine for the villages and evaluated for the presence of blood with a simple dipstick test. But in many cases, a dipstick was not necessary to make a diagnosis because the urine looked almost like pure blood. Anemia is already a significant problem in the tropics because of malaria, hookworm infection, and low dietary intake of meat. Urinary schistosomiasis is yet another factor contributing to the burden of anemia in these villagers.
Fortunately, our mission team was able to provide the drug praziquantel to the infected villagers. For about $10, you could treat a case of schistosomiasis. Of course, they would inevitably get infected again in the future, but for a time, you could arrest the parasite destroying their urinary tract and stop the perpetuation of the infection in the village by eliminating the excretion of the eggs. We were gratified to help the people of one small village overcome one of their many hardships. But over 700 million people live in areas of the globe that are at risk for contracting schistosomiasis. Mass treatment programs, access to safe water, and research into more effective drugs and vaccines are needed to curb the ravages of this parasite on the impoverished peoples of developing countries.
About the author:
Dr. Gregory M. Anstead is an infectious diseases specialist with appointments at the Health Science Center and the South Texas Veterans Healthcare System. Dr. Anstead has been the director and lead clinician of the Infectious Diseases and Immunosuppression Clinics of the South Texas Veterans Health Care System. He has also treated HIV and infectious diseases patients at the Family Focused AIDS Clinical Treatment Services clinic of University Health System since 2000, and has been the clinic’s assistant director since 2011.
[/bgsection]

At long last
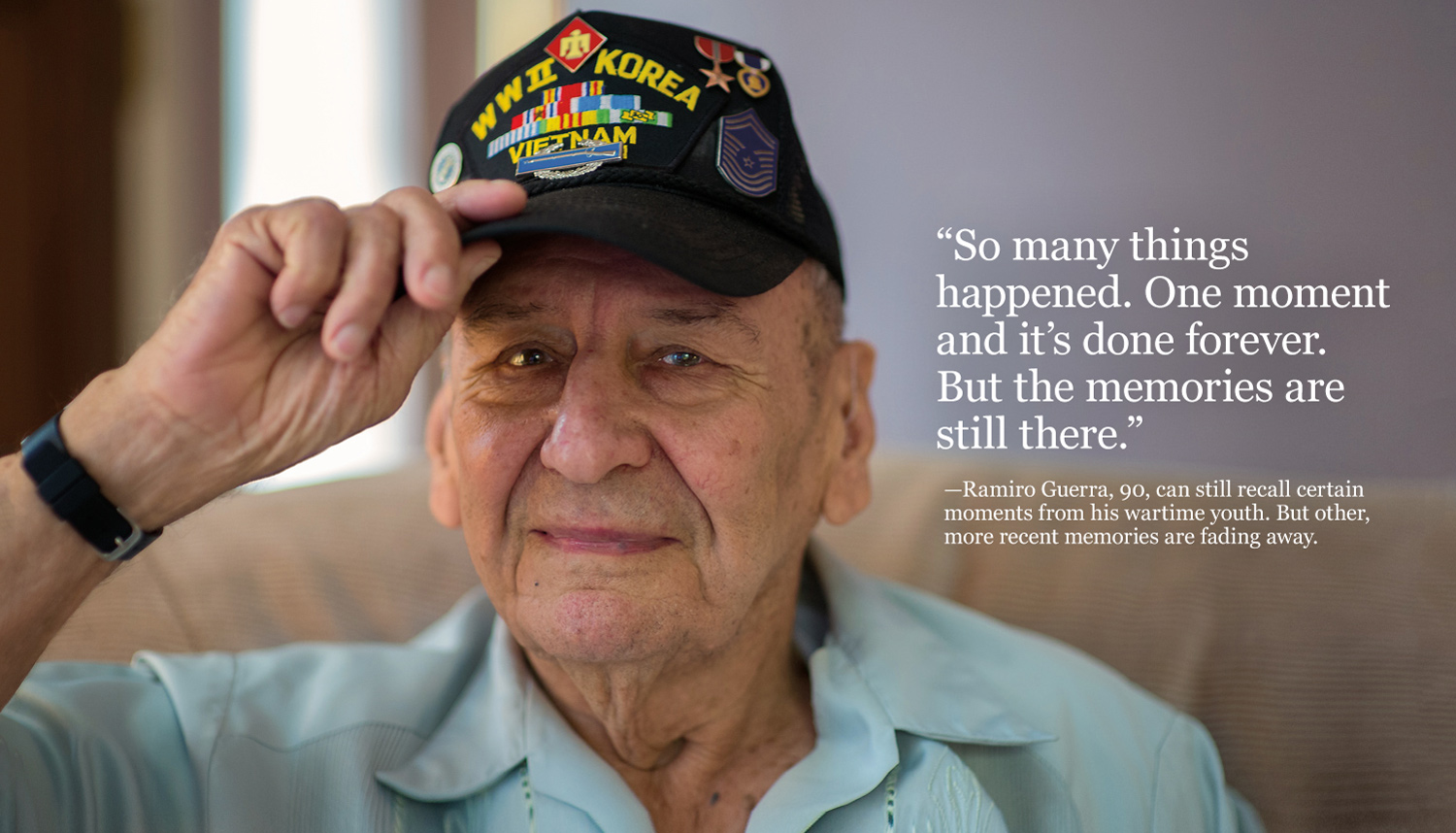
Ramiro Guerra, 90, does yard work whenever the weather’s good. Other times he is inside, often sleeping and sometimes agitated. The U.S. veteran began to forget things in 2006, the year his wife of 57 years, Elida, passed away.
“It seemed like my dad short-circuited,” said his son, Robert Guerra.
The elder Guerra served in Africa, Italy and France in World War II and helped liberate survivors of the Nazi concentration camp at Dachau. He was an Army platoon leader, performed reconnaissance missions and served in three infantry regiments.
In 1948, a year after the Air Force became its own military branch, Guerra enlisted again and served 28 more years, including duty in Korea and Vietnam.
“He did three wars,” Robert Guerra said, and for this Guerra earned Purple Heart and Bronze Star medals.
But it’s a time that his father sometimes struggles to remember.
Described as having a Type A personality, Ramiro Guerra can no longer “connect the dots” cognitively, his son said. “He can see his decline, and it bothers him.”
When asked to join a study of an experimental intervention in human aging involving rapamycin, Guerra “almost insisted he wanted to do it,” his son said.
Rapamycin is the first pharmaceutical intervention shown to extend the life span of middle-aged mice, a finding reported by researchers from the UT Health Science Center’s Barshop Institute for Longevity and Aging Studies and two collaborating institutions in Nature in 2009. Science, Nature and TIME magazine each extolled the finding as one of that year’s top discoveries.
Rapamycin was first proposed as an intervention for aging at the Health Science Center and has been extensively studied in cells and animals at the Health Science Center ever since.
A naturally occurring bacterial product first isolated from soil taken from Easter Island, the base drug rapamycin has long been federally approved to suppress organ rejection in transplant patients.
“We thought, goodness gracious, this is an approved drug. We should be able to do this [trial] fairly quickly,” said Dean L. Kellogg Jr., M.D., Ph.D., professor of medicine and the principal investigator of the rapamycin study.
“But how can researchers study life span in humans? A lot of times, the subjects will live longer than the researchers. So we are looking at proxies for life span.”
The first clinical trial was conducted in 2013 at the Audie L. Murphy Memorial VA Hospital by researchers from the Barshop Institute.
Ramiro Guerra and seven other male veterans, aged 80 to 95 years old and in relatively good health, were immunized for hepatitis B—chosen as a marker to determine an improvement in immune systems. Then the veterans were split into two groups. One group, including Guerra, received rapamycin; the second group received an inactive placebo. The trial lasted four months.
Researchers recorded any changes in the veterans’ physical functions, such as walking speed and hand-grip strength. They also documented changes in their cognitive functions such as decision making, learning and memory. They continue to study antibody responses to see if they were more robust during treatment with rapamycin.
“If we can demonstrate an effect on an age-related process, such as rejuvenating immune function or improving physical or cognitive function, then that will suggest rapamycin has a life-span function, as well,” Dr. Kellogg said.
Rapamycin was approved for use as an immunosuppressant in transplant patients in 1999. For years its value was debated—many scientists thought rapamycin might do as much harm in people as good.
“Rapamycin has been used in transplant patients who are very ill and receive many medications. I have found there is a clinical bias against it, that it causes diabetes or raises lipids [fats in blood]. This is based on studies from transplant patients,” Dr. Kellogg said.
“Very few studies have done work with rapamycin as a single agent in relatively healthy persons,” he said. “We’ve found it to be a well-tolerated drug, and there were no changes in the blood sugars and only a mild increase in triglyceride [lipid] levels, but this change was the same as in the placebo group.”
If clinical trials demonstrate rapamycin’s value as an intervention to improve health span, the drug would then need to gain Food and Drug Administration approval for use in healthy people. Health span refers to the years of good health a person enjoys across the life span.

For Guerra’s family, the rapamycin did make a difference, although it was small.
During the trial, he could again follow plots of TV shows and was more interactive, according to family members. Sadly, the family noticed after the study that the effects went away, although it is not known why, said Dr. Kellogg. That is one of the mysteries Dr. Kellogg hopes to solve as clinical trials continue. He and his team are applying for additional funding to continue the human research.
“It wasn’t a magic pill, but we did see some improvement in his cognitive abilities,” Robert Guerra said. He offered an analogy to describe his father’s daily life:
“When we get up in the morning and start our day, and we begin creating all these memories, we are writing a run-on sentence on a chalkboard all day long, and we can refer back to things,” he said. “In the case of my father, he is writing that sentence with his right hand, but with his left hand he is erasing it as he goes. If he tries to refer back to what he did 10 minutes ago, it’s gone.
“We believe rapamycin might have slowed down his eraser.”
Photos by Lester Rosebrock, Creative Media Services
[bgsection pex_attr_title="How we got here" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-dark-bg" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="000000" pex_attr_textcolor="000000" pex_attr_height=""]
To prove that aging interventions, such as rapamycin, actually work in humans, researchers must first move the science of healthy aging from the idea stage to preclinical and animal studies.
Human clinical trials are at the end of a multi-year, sometimes arduous process.
The Barshop Institute for Longevity and Aging Studies, which opened in 2005 after many years of aging research had been conducted at the UT Health Science Center, is one of the few places in the country that can both investigate the aging process and move the findings into the clinic. As a recipient of the Claude D. Pepper Older American Independence Center grant from the National Institute of Aging (NIA), the Barshop Institute is now comprehensive, said Barshop Institute Director Nicolas Musi, M.D., a physician-scientist in the areas of aging and metabolic disease.
The Pepper Center designation, expected to bring as much as $3.5 million over five years, enables translation of research into practical applications in the lives of older Americans. It joins another NIA award, also totaling $3.5 million over five years. The Health Science Center received a perfect score on its renewal application for the Nathan Shock Center of Excellence in the Biology of Aging. This will provide core services and support for aging research and education.
These new grants ensure that the research geared toward improving how people age will continue and expand over the next several years, Dr. Musi said.

“We will be unique in the country in our capacity to investigate the aging process and move our findings into the clinic,” he said.
The Barshop Institute became one of a handful of centers in the country to have a Shock Center in 1995, and has maintained the designation ever since, receiving more than $18 million in funding.
“A very small number of these centers are able to secure the NIA Shock Center funding,” Dr. Musi said. “It is the equivalent of a National Cancer Institute designated cancer center in terms of stature in the world of aging research.”
The Barshop Institute is also one of only three centers in the NIA Interventions Testing Program and last year received funding of $7.5 million through 2019. With the renewal of the Geriatric Research, Education and Clinical Center designation within the South Texas Veterans Health Care System, also received last year, the Barshop Institute has all four sought-after designations.
[/bgsection]
[bgsection pex_attr_title="Living livelier" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-dark-bg" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="000000" pex_attr_textcolor="000000" pex_attr_height=""]
 For a picture of productive, healthy aging, U.S. Air Force veteran Allie Burton’s progeny need look no further than their family patriarch. The Barshop Institute for Longevity and Aging Studies at the UT Health Science Center is even looking at the fitness of this rural Texan.
For a picture of productive, healthy aging, U.S. Air Force veteran Allie Burton’s progeny need look no further than their family patriarch. The Barshop Institute for Longevity and Aging Studies at the UT Health Science Center is even looking at the fitness of this rural Texan.
At 91 years old, Burton is running 15 head of cattle at his 500-acre ranch near Junction, Texas. In the late fall, he’ll take his cattle to market about 60 miles east in Fredericksburg.
“I raise exotic game and cattle and at times take goats out there,” he said. “It keeps me busy; there’s always something to do. It keeps me physically active.”
Burton was among the first eight veterans to participate in a clinical research study of the drug rapamycin. The study, conducted by the Barshop Institute and the South Texas Veterans Health Care System, is testing the drug as a possible intervention for aging. Dean Kellogg, M.D., Ph.D., and other faculty in the Long School of Medicine are studying test results from Burton and the other veterans to assess whether rapamycin improved their physical ability, immune system function, and learning and memory.
“I happened to go down to the San Antonio VA to a prisoner-of-war clinic,” Burton said. “While I was there, Dr. Kellogg came up and told me something about the study and asked if I would be interested. I said yes, if it would make me livelier.”
Burton served 23 years in active duty in the Air Force and five in the Air Force Reserves. He went through pilot training during World War II and was disappointed to be assigned to the training command as an instructor.
“I wanted to be in the sky, like Snoopy chasing the Red Baron,” he said.
During the Korean War, he got his wish. But while flying an F-84 fighter-bomber, he was shot down by anti-aircraft fire. The loneliest and coldest winter of his life ensued.
Burton was a POW from 1952 to 1953.
“I was a guest of the Chinese Communists for 10 months,” he said. “It was way up north, just across the Yalu River from China. It is very cold up there—I always thought that’s where Admiral Byrd [Richard Byrd, 1888-1957] went to train for his cold-weather operations at the South Pole.”
After his release in 1953, he returned to his hometown of Kerrville, Texas. The 29-year-old war hero was welcomed with a parade, where, incidentally, he would meet his future wife, Betty, for the first time.
“I’ve known him since I was 9,” said Betty Burton. “My father said, ‘We’re going to see this local man who came home.’ I remember that day.”
After his active duty, Allie Burton retired in Kerrville and became a real estate broker. He realized his lifelong dream when he was able to buy the ranch, in addition to a house in Ingram where he stays when not at the ranch.
He and Betty were married in 1997—44 years after they met. He has two children and she has three. Together they have nine grandchildren and six great-grandchildren.
“We have ’em every day. Someone is always here,” he said.
Allie Burton is a dancer who always walks fast, his wife said. They enjoy country dancing in area dance halls, from Bandera to Fredericksburg to Hunt.
But last year, there was a change in her husband, Betty Burton said. He was lying down two to three times during the day because he was tired.
“After taking rapamycin for a length of time, he quit lying down so often,” she said.
It’s impossible to base a therapy for aging on anecdotal stories. Dr. Kellogg pointed out that only a few volunteers have received the drug, and more study is needed. He and other School of Medicine researchers are seeking additional funding to expand the study.
The Burtons agree that whatever is learned about rapamycin will prove to be important.
“I would like to think that I can help humanity in some way, if that’s what it comes to, and that my grandkids and great-grandkids could benefit from that,” Allie Burton said.
[/bgsection]
[bgsection pex_attr_title="Barshop Institute" pex_attr_subtitle="Through the years" pex_attr_undefined="undefined" pex_attr_style="section-dark-bg" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="000000" pex_attr_textcolor="000000" pex_attr_height=""]
1970s, 80s and 90s – Research in basic science departments of the Health Science Center includes a strong focus on dietary calorie restriction and its effects on aging in mice, conducted by pioneers such as Edward J. Masoro, Ph.D.
1992 – The Aging Research and Education Center (AREC), the forerunner of today’s Barshop Institute, is established. Arlan G. Richardson, Ph.D., was the founding director.
1995 – The AREC is one of the first centers in the country to be named a Nathan Shock Center of Excellence in the Biology of Aging, a designation the Barshop Institute retains today. Shock Centers are funded by the National Institute on Aging (NIA) of the National Institutes of Health. They provide leadership in the pursuit of basic research into the biology of aging.
2001 – The University of Texas System Board of Regents approves the honorific name: The Sam and Ann Barshop Institute for Longevity and Aging Studies. Mr. Barshop served on the Board of Regents previously, and he and Mrs. Barshop were generous donors to aging research at the Health Science Center. Other donors to the institute included The Brown Foundation Inc. and the UT System.
2004 – The NIA selects three U.S. centers, including the Barshop Institute, to participate in the NIA Interventions Testing Program (ITP). The centers investigate treatments that have the potential to extend life span and delay disease and dysfunction in mice. Randy Strong, Ph.D., is principal investigator of the ITP at the Barshop Institute.
2004 – A Health Science Center researcher, Z. Dave Sharp, Ph.D., proposes rapamycin, a medication used in transplant and other patients, to be studied in the ITP. Dr. Sharp later wins the Mprize Lifespan Achievement Award from the Methuselah Foundation for his foundational ideas about rapamycin’s potential effects in aging.
2005 – The Barshop Institute building is dedicated. Mr. and Mrs. Barshop are joined by keynote speaker Sen. Kay Bailey Hutchison and many faculty and dignitaries for the celebration.
2005 – Drs. Strong and Sharp run into a problem studying rapamycin: It is not stable enough in food to register in the blood level of mice. This causes a delay in the mouse studies. Dr. Strong works with Southwest Research Institute to microencapsulate rapamycin, making it feasible to do animal studies. Because of the delay, rapamycin is studied in mice that are 20 months old – the equivalent of 60 years of age in humans.
2009 – Results of the ITP study of rapamycin in mice of both sexes are published in the prestigious journal Nature. The rapamycin formulation developed by Dr. Strong extends the maximum life span of the middle-aged mice by 28 percent to 38 percent. This is the first pharmaceutical intervention shown to extend longevity in mice; previously only dietary calorie restriction and genetic manipulation had been successful.
2010 – Veronica Galvan, Ph.D., of the Health Science Center, publishes results showing that administration of rapamycin improves learning and memory in a strain of mice engineered to develop Alzheimer’s-like deficits.
2013 – Rapamycin enters human clinical trials, with four military veterans receiving the drug and another four receiving a placebo. Nicolas Musi, M.D., is named director of the Barshop Institute.
2014 – The Barshop Institute receives renewals of the NIA Interventions Testing Program and the Geriatric Research, Education and Clinical Center. The GRECC is within the South Texas Veterans Health Care System.
2015 – Dr. Musi announces the Barshop Institute’s first NIA Claude Pepper Center designation and a perfect score on the application for competitive renewal of the NIA Nathan Shock Center. Dr. Strong is the Shock Center director and Peter Hornsby, Ph.D., is co-director.
[/bgsection]

Pursuing concussion’s cure
 Veronica Carrillo, 17, and her mother, Paula, waited in the emergency department at University Hospital for the doctor’s diagnosis. The avid soccer midfielder had gone up to head the ball in a game when, in midair, the side of her head collided with the forehead of another player. Skulls are hard; no ball could make that kind of impact.
Veronica Carrillo, 17, and her mother, Paula, waited in the emergency department at University Hospital for the doctor’s diagnosis. The avid soccer midfielder had gone up to head the ball in a game when, in midair, the side of her head collided with the forehead of another player. Skulls are hard; no ball could make that kind of impact.
“I felt dizzy but kept going,” Veronica said. “I didn’t stop until I tried to head the ball again; I headed it wrong, with the top of my head, and I had a period of time when I didn’t know what was going on. They told me I blacked out.
“I thought I was going to get better, so I just went home and stayed there. I started getting really bad headaches, but I’m hardheaded and went and played again a couple of days later. After that game, I felt really bad. I had headaches and started throwing up. I’ve been throwing up since then [for three days].”
Concussions happen every day, everywhere, to anyone, and they happen in so many ways:
Your toddler, who’s interested in everything, reaches for the unanchored TV set, which falls and slams into her head. You’re filled with fear as you agonize about her developing brain.
Your son, the high school football jock, takes a helmet-to-helmet hit. The players climb off the pile, and you realize that the one who lies limp and immobile on the field is your son. The world stops as you see him carried off the field.
Your mother, 85, who still insists on doing things for herself, falls on loose floor tiles. You see closed eyes and a trickle of blood, and you realize she has hit her head. You frantically call 911, wondering what this will mean for the weeks and months ahead.
“I see head injuries every day in the emergency department, and the age range varies from small infants to 90-year-old people who trip and fall,” said Christopher Gelabert, M.D., assistant professor in the Department of Emergency Medicine and physician with UT Health San Antonio. “The most common is probably a slip and fall from a standing height.”
A concussion is a type of brain injury that temporarily stops the brain’s functions. It is commonly described as “getting your bell rung” and “seeing stars.” These casual terms may make the condition sound minor, but concussions are serious. Symptoms can range from a nagging headache to seizures, bleeding in and around the brain, and death.
“What we’ve done in sports medicine is to try to separate the word ‘mild’ from ‘severe’ in a concussion diagnosis,” said Rudy R. Navarro, M.D., assistant professor in the Department of Family and Community Medicine and family physician with UT Medicine. “This is because all concussions are treated the same way, currently, and secondly we don’t have a way to really determine what’s mild or severe or chronic until after the fact.”
Unlike cuts, there is no way to treat a concussion with a Band-Aid. The injury is within the skull, and it isn’t healed readily. Rest and observation are the recommended ways to treat a concussion today, but with an injury like this, they may not be enough.
“Any concussion has the potential to be a serious concussion,” Dr. Navarro said. “A person can develop myriad symptoms, including headaches, dizziness, fatigue, lightheadedness and loss of balance, as well as cognitive issues such as short-term memory impairment, increased time to learn new concepts, and difficulty retaining information. These effects may be developed over days, weeks and even months.”
Over the long term, repeated injuries could be associated with the early onset of degenerative brain diseases, as the public is learning through stories of former National Football League players such as Hall of Fame running back Tony Dorsett of the Dallas Cowboys, who was diagnosed with chronic traumatic encephalopathy. The disease is associated with memory loss and confusion, as well as problems with impulse control, aggression and depression. Eventually, it leads to dementia.
“During football season, we see more head injuries in young people,” Dr. Gelabert said. “Parents are very concerned, with all the things you see on TV with the NFL.”
A potential answer
But what if the brain, the seat of reasoning, memory and emotion, could be stimulated to heal itself? Researchers in the School of Medicine have discovered a possible avenue to do just that, and it lies—appropriately—within the brain’s so-called “caretaker” cells, called astrocytes.
The skull is a confined space, and the brain rests inside it in a bath of cerebrospinal fluid. When a concussion occurs, the brain is temporarily and violently shifted. Swelling from fluid retained in the brain tissues, called edema, creates pressure in the confined area. This can lead to the death of neurons—cells that signal nerves throughout the central nervous system to do all of life’s functions.
The research centers on a class of compounds called purinergic receptor agonists.
James D. Lechleiter, Ph.D., professor in the Department of Cellular and Structural Biology, has found that treating the astrocytes with the agonist compounds can stimulate the caretaker cells to be more active—essentially giving them a kick-start to minimize the swelling.
[bgsection pex_attr_title="" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="" pex_attr_image="https://magazines.uthscsa.edu/mission/wp-content/uploads/sites/20/2015/06/concussion_illustration.jpg" pex_attr_imageopacity="1" pex_attr_bgimagestyle="static" pex_attr_titlecolor="ffffff" pex_attr_textcolor="ffffff" pex_attr_height="500"]When a concussion occurs,
the brain is temporarily
and violently shifted. Swelling
creates pressure in the
confined area and can lead
to the death of neurons.
Researchers have found that
stimulating astrocytes, the
so-called caretaker cells,
with agonist compounds
could kickstart a reduction
in swelling.[/bgsection]
Illustration by Sam Newman, Creative Media Services
The effects are significant. In the brains of live mice, treatment of the astrocytes with the compounds consistently and dramatically reduced neuron death. The results also held true in the first trial on human brain tissue, obtained from patients who underwent surgery for epilepsy.
“We hope to limit and even reverse the effects of concussions,” Dr. Lechleiter said. “Essentially, we think we can enhance the brain’s ability to heal itself.”
Dr. Lechleiter received a U.S. patent for the discovery of the compounds’ benefits at the close of 2013.
He endured a lengthy process—seven years—replete with rejections and arguments. The UT Health Science Center technology commercialization team helped him in this effort.
“You get three strikes and you’re supposed to be out,” he said. “In this case we had at least four strikes but prevailed. When you’re developing something, you have to believe in it. We’re very excited about the clinical impact of our findings and hope this success leads to new drug therapies for people with multiple types of brain injuries.”
According to the Centers for Disease Control and Prevention, an estimated 1.7 million people sustain a traumatic brain injury annually. About 75 percent of these are concussions or other milder forms of brain injury. Children 4 and younger, adolescents 15 to 19, and adults 65 and older are at greatest risk, CDC statistics show. Head injuries result in more than 1 million emergency department visits per year.
“A concussion can happen at any age,” Dr. Navarro said. “The symptoms can be very subtle and can be masked by other disease processes. Also, if a patient has a significant traumatic injury or fracture and is on pain medicine, what may be completely missed, not even considered, is that the patient had a concussion.”
In toddlers and older developing children under the age of 12, the symptoms can be subtle and unusual, and are commonly missed. These symptoms can include irritability, excessive crying, a change in eating or sleeping patterns, loss of balance and appearing dazed or listless.
“That is a difficult group in which to make the diagnosis, because their symptoms are very different from what we see in teenagers and adults,” Dr. Navarro said. An added complication is younger children often can’t articulate what they’re feeling.
The elderly are susceptible to falls and, by extension, concussions.
“We worry in this group about hemorrhages, stroke, fracture and vitamin D deficiency, but sometimes we forget. We don’t step back and say this might be a concussion,” Dr. Navarro said. “There are so many confounding factors that it is difficult to treat.”
Medical science has miles to go in learning how to treat concussions. Rest is usually advised, along with ceasing sports and other activities that increase the risk of a second injury and refraining from activities such as schoolwork and computer use that require thinking and concentration.
In each age group, when a concussion is suspected, a medication based on stimulation of the caretaker astrocyte cells could be a true breakthrough, Dr. Navarro said.
“A treatment that could help prevent immediate or long-term complications, especially the cognitive issues, would be tremendous,” Dr. Navarro said. “We would have to show it makes a significant difference in patients’ lives, more than what we are doing now. We need to truly define the effects of concussion down the road. If we find that these injuries cause dementia or psychiatric issues long term, then any kind of treatment that is an adjunct to current care would absolutely be novel and groundbreaking.”
Promising beginning
The earliest preclinical testing of the therapy is complete, and Dr. Lechleiter, the Health Science Center and his new start-up company, Astrocyte Pharmaceuticals Inc., seek to move the program into different animal models, and ultimately to Food and Drug Administration trials in humans.
“We are at a stage where we know we have a molecule that works,” Dr. Lechleiter said. “The plan is to make small modifications to see what works the best. Once we have the molecule we want, we will enter a subcontract to test it in small animals.”
It is difficult to predict how many years it might be before this therapy could be widely available to the public.
“Right now the delivery method is uncertain,” Dr. Lechleiter said. “Clinical trials may test intravenous injections. It could later be sublingual, and melt in your mouth. We don’t know at this time.”
Animal studies and then human clinical research must show that the benefits of receiving an astrocyte stimulator for a concussion greatly outweigh any possible risks.
Things often move slowly in drug development. But if it takes 10 years or 20 years, it will be worth it, Dr. Lechleiter said, because the applications are enormous—from a toddler’s accident to the battlefield in Iraq.
And, of course, to the sports field.
The day of Veronica Carrillo’s visit to the hospital, nothing was more important than learning the extent of her head injury and what could be done. It was a minor concussion; rest and cessation of activities were prescribed. But what if a safe, effective infusion of astrocyte therapy had been available for a nurse or physician to administer?
“I feel like if I had taken a pill or something, it would have healed me sooner, and I could have played again sooner,” she said a week later.
Her future rides on her getting back on the field. The South San Antonio High School graduate has a scholarship to play for the Larks women’s soccer team at Hesston College, located about 35 miles north of Wichita, Kansas.
Will she do headers during games? “Oh yes,” she said without hesitation. “I am going to play like I’ve always played—strong—I’m still going to do headers and everything.”
She could be just one game away from her next concussion, but that’s a risk she’s willing to take, she said.
In the future, if Dr. Lechleiter’s astrocyte therapy proves successful and is available to emergency responders, someone at such a game could call 911, and the player could either receive the medication at the field or after arriving at a local hospital.
This is the future of medicine Dr. Lechleiter envisions.
“We don’t want to get ahead of where we are with the science,” he said, “but no other options are available to treat concussions at the moment, so any novel effective therapy is going to be a blockbuster. It would be used in emergency rooms and ambulances, in primary care and in any place with trained medical personnel. With professional supervision of this very powerful medicine, we could relieve not only the immediate effects of concussions but prevent many of the long-term effects, too.”

Window to the brain
 In a flap of skull the size of a pinhead, Martin Paukert, M.D., mounts and seals a thin window onto an anesthetized mouse.
In a flap of skull the size of a pinhead, Martin Paukert, M.D., mounts and seals a thin window onto an anesthetized mouse.This window will allow Dr. Paukert and his team to monitor, in real time, effects of stimuli to the brain of a conscious mouse while it walks on a tiny treadmill. That’s something that’s not often done, Dr. Paukert said, but that can yield important data.
Dr. Paukert is the principal investigator of a five-year, $2 million grant from The Robert J. Kleberg, Jr. and Helen C. Kleberg Foundation to study brain activity that may take place long before Alzheimer’s disease symptoms are observed.
“The unraveling of the mystery of this terrible illness will emanate from discoveries along the lines of what Dr. Paukert and his colleagues are doing,” said UT Health Science Center President William L. Henrich, M.D., MACP. “You can’t develop a drug, you can’t develop an antibody, you can’t develop something to prevent this unless you know what lies at the very center of the problem. That’s why this work is so important. The consequences of having a neurodegenerative disease are deeply felt by everybody.”
One of the earliest sites of noticeable neurodegeneration is a brain stem structure called the locus coeruleus. This structure has a major influence on the entire central nervous system because it delivers norepinephrine, a neurotransmitter associated with attention or arousal. Initial triggers of Alzheimer’s disease may include less norepinephrine release, and fewer norepinephrine-dependent calcium spikes in cells called astrocytes. While astrocytes are the major support cells for neurons, in Alzheimer’s this relationship appears to be somehow affected, causing the death of neurons.
Using Dr. Paukert’s system, the scientists measure spikes in calcium signaling in the astrocytes, which occur when the mouse walks on a treadmill or, more pronounced, when the mouse follows the movement of the motorized belt of the treadmill. During the measurements, the mouse is conscious and the window to its brain is immobilized under the microscope. Critically, its legs remain free to walk.
“This technique gives us a window into how brain cells engage in a cross-talk and how these communications are determined and interpreted by a certain behavior,” said Dr. Paukert, assistant professor of physiology. “The hope is that we can use these signals as a readout of what is necessary to normalize norepinephrine signaling, and to see whether this intervention slows the progression of Alzheimer’s disease.”
Only a handful of labs around the world are recording these spikes in real time, while the mice are awake, said Manzoor Bhat, Ph.D., professor and chairman of the Department of Physiology.
“The Paukert lab is in its early phases in San Antonio, and funding from The Robert J. Kleberg, Jr. and Helen C. Kleberg Foundation will have a major impact on how quickly they can get the animal models established to address the central questions related to the early onset and progression of Alzheimer’s disease in real time,” Dr. Bhat said. “In the future, this will allow exploration of new avenues for therapeutic intervention.”

When the shock wave hits
Imagine you are a soldier, patrolling the streets of a war-ravaged city. Without warning, a suicide bomber sets off an improvised explosive device 50 yards from where you stand. The powerful blast flips you backward into a wall. In seconds you open your eyes. How are you seeing? Will this affect your vision permanently?
Researchers from the joint biomedical engineering program of the Health Science Center and The University of Texas at San Antonio have evidence that eyes subjected to that kind of pressure, even if not punctured, are seriously injured and could suffer partial or complete blindness.
In 2014, the team published a study of blast effects in a postmortem pig eye model. For two years, researchers tested blasts contained inside a tube system at the U.S. Army Institute for Surgical Research, located on Fort Sam Houston in the San Antonio Military Medical Center complex. The U.S. Department of Defense funded the study.
Postmortem pig eyes were exposed to various levels of blast energy and were evaluated with photography, ultrasound and microscopic examinations. Researchers found that an initial shock wave of over-pressurized air from a blast is enough to damage the eyes, even in the absence of shrapnel or other particles. The optic nerve, which serves as the conduit of messages between the eyes and the brain, can also be damaged, leading to numerous visual deficits.
The study is crucial given the dangers soldiers face today. During the Civil War, 1 percent of battlefield injuries involved the eye; this increased to 3 percent through World War II. During the last several combats in the Middle East, 13 percent of injuries have involved the eye. Ocular injuries are now the fourth most common military-deployment injury.
“We think it’s largely due to the use of explosive devices,” said study co-author Randolph Glickman, Ph.D., professor of ophthalmology and radiological sciences in the School of Medicine at the Health Science Center. “They are everywhere, they are messy devices, and they produce lots of eye injuries.”
The problem is not restricted to the battlefield. Each year, 2.4 million eye injuries occur in the U.S. A fifth of Americans will experience one in their lifetime, ranging from a scratched cornea to loss of vision. Ocular trauma is the leading cause of blindness in the U.S.
“Obviously it’s a serious issue in both the military and civilian communities,” said Dr. Glickman, who is cross-appointed at UTSA in physics and biomedical engineering.
Blast injuries can be categorized in four levels: primary, resulting from the pressure wave produced by the blast itself; secondary, due to shrapnel or debris thrown up by the explosion; tertiary, concussive injuries resulting from the whole body being thrown forcefully against a solid object; or quaternary, long-term effects such as post-traumatic stress disorder.
The blast wave hits people so fast that they don’t have time to blink for protection, and even low blast levels can cause eye damage.
The work came out of a pilot study of paintball injuries by geologist Walter Gray, Ph.D., and ophthalmologist Rick Sponsel, M.D., both faculty at UTSA. The researchers found that computer models used by engineers to evaluate how materials break under mechanical stress could also be used to predict eye injuries sustained from different levels of trauma. The machine is so correct, they found, that the type and severity of injury predicted by the computer model matched the actual injuries sustained in lab trials using animal eyes.
Dr. Glickman uses the information to investigate the biological responses to blast trauma.
Before the research, this damage to the eyes was frequently attributed to traumatic brain injuries.
“Internal effects in the eye are something no one has really studied,” said co-author Matthew Reilly, Ph.D., assistant professor of biomedical engineering at UTSA. “Previous studies looked at whether the eye ruptured during the secondary stage, but those research teams didn’t have the sophisticated equipment to look at the inside. In this study, we’ve been able to distinguish between primary and secondary blast effects.”
With the primary blast, the pressure is more widely distributed, Dr. Reilly said.
“The pressure’s not hitting at one point on the eye but across the whole surface,” he said. “The eye isn’t punctured at this step, but the soft parts inside the eye get scrambled. Bad things happen.”
The research team observed retinal detachments, separation of tissue layers, optic nerve damage and injuries to a group of structures that help maintain fluid and pressure balance in the eye.
Those things don’t have to happen, the researchers said. Existing eyewear shields against objects such as shrapnel but doesn’t address blast waves. In the future, they would like to collaborate with Department of Defense specialists to design new types of protective eyewear. Blast modeling would lead to development of prototypes that could be tested to determine which designs best prevent primary blast injuries.
Over time, the project could also help physicians better screen patients for ocular damage and create appropriate treatment plans for the increasing number of soldiers who suffer eye blast injuries while in harm’s way.

A father's gift
Before Jackson Pineda was born, doctors told his parents, Gerald and Jennifer, that their son’s kidneys would not last past the age of 10. A prenatal ultrasound showed one enlarged kidney and the other, they believed, would not be strong enough to make up the difference.
To the couple’s amazement, the doctors’ forecast proved accurate almost to the day.
Doctors had removed the enlarged kidney when Jackson was 2 years old, and his remaining kidney functioned at only half of healthy capacity. By age 4, kidney insufficiency prevented Jackson from growing normally, and daily injections of growth hormone became a way of life.
On Nov. 6, 2010, two days short of his 10th birthday, University Transplant Centersurgeons removed one of Gerald Pineda’s kidneys and placed it in his son’s body.
"We never gave it a second thought," said Gerald Pineda. For years he had known he was a good match to be a donor for his second-oldest son, whenever the time came.
With the transplant center’s Robert Esterl, M.D., leading the team performing Jackson’s surgery, and Kenneth Washburn, M.D., professor of surgery in the Long School of Medicine, leading Gerald Pineda’s team, the transplant took three hours. It was a success.
The University Transplant Center, a clinical partnership of the Health Science Center and the University Health System, offers one of the only pediatric kidney transplant programs in the region. The one-year survival rate for University Transplant Center pediatric kidney patients is 100 percent, according to the Scientific Registry of Transplant Recipients. The one-year survival rate of adult kidney recipients, 94.8 percent, surpasses the national average.
The center also has one-year patient survival rates that exceed national rates in two other signature services, with 85.1 percent for lung transplants and 94.1 percent for liver transplants. The team is the only one in San Antonio to offer the option of living-donor liver transplants.
"I’m very happy with where the University Transplant Center is today," said Glenn Halff, M.D., professor of transplant surgery and director of the center. "It has grown into a mature program that continues to refine the quality of care and medical treatment options that we provide."
Living-donor organs enable children and adults to receive transplants sooner, Dr. Halff said. Roughly 30 percent of transplants at University Hospital involve live donors such as Gerald Pineda. That’s a number the doctors would like to see increase, said Greg Abrahamian, M.D., associate professor of surgery in the Health Science Center's School of Medicine and surgical director of the kidney transplant program.
"We would like to get that up to 50 percent, because the wait time without a living donor is roughly six years in our region," Dr. Abrahamian said. "With living donors, many patients can be transplanted before having to go through dialysis."
That was the case for Jackson.
"He never had to have dialysis because he had a living donor," Jennifer Pineda said. "My husband was willing and able, and spared Jackson from it. We were so fortunate."
And since the majority of kidney donor surgeries are laparoscopic, with only a small incision needed for the donated kidney to be removed, the recovery for Gerald Pineda had resulted in less post-operative pain, a quicker recovery and a shorter time in the hospital.
Both father and son healed well immediately after the transplant, but two months after receiving his new kidney, Jackson was afflicted with a virus infection called BK, which frequently occurs in organ transplant patients and can cause progressive kidneydamage.His nephrologist at the time, Mazen Arar, M.D., medical director of pediatric nephrology with the University Transplant Center, said it was the worst case of BK virus that he’d ever seen, leading to Jackson’s eventual readmission to the hospital with dangerously high blood pressure.
"That was the scariest moment," Gerald Pineda said. "We had this good kidney that we had given him—and we were in danger of losing it."
Thankfully, Jackson’s body responded to treatment. His blood pressure stabilized and his health returned.
Jackson is now 13 and a member of his seventh-grade golf team at San Antonio’s Hector Garcia Middle School. He recently shot a nine-over-par 38 on nine holes, leading all players in a middle school tournament. His skills extend to the fine arts, as well. This year he was recognized as one of the state’s best pianists in his age group.
He’s mellow and carefree, his parents said. And father and son have a few other things in common.
"He loves golf, just like me," Gerald Pineda said. "Whether a shot is good or bad, you can’t tell whether he’s upset."
They don’t talk much about Jackson’s rocky first years. There’s really no need to.
"He’s so normal, you would never know that he had a bad kidney," Gerald Pineda said. "We don’t talk about it very much at all. It’s just part of life."

It takes a team
The University Transplant Center is a clinical and academic partnership with transplants performed at University Hospital by physicians from UT Health San Antonio, the faculty practice of the Long School of Medicine at the UT Health Science Center San Antonio.
"We have an exceptionally knowledgeable and skillful faculty," said Glenn Halff, M.D.,Dielmann Chair in Transplant Sciences, professor of transplant surgery and director of the center. "The team works in a unique multidisciplinary environment that optimizes patient care."
Surgeons include:
- Robert Esterl, M.D.
- Kenneth Washburn, M.D., Valero President’s Distinguished Chair in Transplantation
- Greg Abrahamian, M.D., Joan Wish Endowed Professorship in Transplant Surgery
- Francisco G. Cigarroa, M.D., chancellor of The University of Texas System, who will return full time to the University Transplant Center once his successor as chancellor is named.
The surgeons collaborate with a team of pediatric nephrologists and hepatologists:
- Mazen Arar, M.D.
- Daniel Ranch, M.D.
- Ikuyo Yamaguchi, M.D., Ph.D.
- Naveen Mittal, M.D.
- Jaime Echartea Gonzalez, M.D.
Dr. Halff said the University Transplant Center is successful because of its many partnerships and collaborations.
"Our outcomes are excellent," he said. "For patients who live in this region of Texas, there is no reason to go anywhere else."
An estimated 1,000 South Texans are on the organ recipient wait list. To sign up as an organ donor, go to donatelifetexas.org or call 1-888-336-9633.

Big relief through a hole the size of a dime
Nanette Hathaway well remembers when the pain began. It was Christmas 2009, and she had flown down from Seattle, Wash., to visit her daughter in San Antonio.
"I was in bed when a sharp pain hit my vocal cords and never went away," she said. "The pain was so strong that I couldn’t talk for the whole vacation. I thought it was a flu or something. I went to a pain management place and they guessed it was neuralgia. I kept yelling, help me, help me get rid of this pain."
Doctors put her on hydromorphone, a narcotic analgesic, but the medicine only masked the pain.
"It was like I drank acid through my mouth," she said. "It was the worst pain in the whole world, and eventually it made me want to commit suicide. I lived through it for my children because I always asked myself, what would happen if I did commit suicide? They would have to live with it."
She coped with the pain for four years. Neurosurgeons and ear, nose and throat doctors sent her away with medications and referrals. Then in September 2013, two months after she permanently moved to San Antonio, Hathaway broke her neck in a traffic accident. She was taken to University Hospital where she met David F. Jimenez, M.D., FACS, professor and chairman of the Department of Neurosurgery in the Long School of Medicine at the UT Health Science Center San Antonio.
He repaired her neck, but her vocal cord pain continued. After more rounds of medications and referrals, she returned to Dr. Jimenez for help.
"He looked at an MRI of the brain and showed me where it was abnormal," she said. "He kept me there for at least an hour, showing me all the pictures. He explained it all to me."
A large blood vessel had shifted over her brain stem and was touching a nerve with every pulse of blood. It was fixable, Dr. Jimenez said, and surgery would be minimally invasive.
On March 3, through a hole the size of a dime and with instruments the size of a pencil lead, Dr. Jimenez finally relieved her pain.
A new generation
From the brain to the hands, neurosurgical procedures are going the way of the endoscope, and Department of Neurosurgery faculty members are routinely performing these surgeries at St. Luke’s Baptist Hospital and University Hospital.
Dr. Jimenez is an internationally recognized expert at the neurosurgical use of endoscopy, which offers an internal view of the body using a flexible tube with a small camera attached at the tip. He also is editor of Intracranial Endoscopic Neurosurgery, a textbook published by the American Association of Neurosurgical Surgeons. He wrote three chapters of the book, including one with his wife, Constance M. Barone, M.D., FACS, on endoscopy-assisted surgeries for the management of craniosynostosis.
"Endoscopy is an important and interesting area in neurosurgery today," Dr. Jimenez said. "Instead of performing a full craniotomy with a large bone flap and scar from ear to ear, we can access an area of interest through a hole the size of a dime. We are able to do things inside the brain and spinal cord to alleviate suffering and improve lives. The hole is repaired with a tiny titanium plate that is as thin as a piece of paper but is not vulnerable. The patient can live worry free."
Dr. Jimenez and Dr. Barone, who joined the Health Science Center in 2004 from the University of Missouri, pioneered endoscopic surgery for craniosynostosis, the premature closing of one or more sutures on a baby’s skull. The brain triples in size from birth to 3 years of age and grows tremendously fast in the first six months. To accommodate this expansion, the skull has five elastic sutures, or seams. If even one of the sutures is closed in the womb or at birth, headaches, eye problems and permanent disfigurement can result. The disfigurement occurs because the brain presses on other parts of the skull, resulting in elongation of the head, a bulging forehead and other deformities.
Before endoscopy-assisted craniectomies for craniosynostosis, babies went untreated or their skulls were opened from ear to ear. Dr. Jimenez said the technique remains largely the same, but a new set of endoscopic instrumentation is making it even better. The operation, which once took two hours, is shorter, easier and safer. To date, Dr. Jimenez, Dr. Barone and their surgical teams have treated more than 600 children.
These less-invasive endoscopic approaches help another high-risk population—the elderly.
Dr. Jimenez operated on a 96-year-old woman who could no longer walk to her mailbox because of pain in her back that radiated down to her legs. She had spinal stenosis, a narrowing of the open spaces within the spine that puts pressure on the nerves of the spinal cord. This results in pain, numbness and muscle weakness.
After a short surgery, her pain was eliminated almost instantly, Dr. Jimenez said. Within a month, she was back to bowling and dancing with her boyfriend.
"Traditional surgery is associated with higher risks for elderly patients," Dr. Jimenez said. "Minimally invasive surgery provides an excellent option for this population of patients who otherwise would not be treated and would have to suffer in pain, as was the case with my patient until she had the surgery."
People with carpal tunnel syndrome are experiencing relief through endoscopy, too. In patients suffering from carpel tunnel, the carpal ligament that connects the hand bones becomes thickened and hard through repetitive use such as typing, and this compresses the median nerve, which runs from the spinal cord down to the fingers. This pressure results in severe pain, tingling, numbness and weakness in the palm and ring finger, sometimes extending into the arm, Dr. Jimenez said.
Historically, carpal tunnel release was accomplished with an incision several inches long. Because the hand is very highly sensitive and nerve-rich, patients faced a six- to eight-week recovery with considerable pain. But Dr. Jimenez can free the carpal tunnel through two tiny incisions, inserting a special endoscope. The pain is greatly reduced, and patients recover in one to two weeks.
"I’ve worked on administrators who had endoscopic surgery on a Thursday and went back to work the following Monday," said Dr. Jimenez, who has performed endoscopic carpel tunnel releases for 20 years.
Patients who have had both procedures—open surgery on one hand and endoscopic surgery on the other—said the endoscopic procedure is overwhelmingly better.
"I’ve had a lot of patients who suffered for years, who then had the endoscopy and kicked themselves for waiting," Dr. Jimenez said.
The Department of Neurosurgery is training a new generation of neurosurgeons, and action in 2014 by the Accreditation Council for Graduate Medical Education approved the expansion of the department’s residency program to 17 residents, one of the largest neurosurgery residency programs in the country. Endoscopies are part of their training.
"Every resident who leaves here is capable of doing these surgeries," Dr. Jimenez said, noting that he is establishing the Center for Neurosurgical Endoscopy by July to further education, research and patient care using the minimally invasive approaches.
For patients, this training will be invaluable, he said.
"If you were given the option of having a very invasive and long surgery," Dr. Jimenez asked, "versus one that involves making a hole the size of a dime, what would you rather have?"
A new life
Months removed from her endoscopic surgery, Nanette Hathaway’s outlook is remarkably changed. For the first time in years, the acid feeling in her mouth is gone. She said she is starting to date for the first time in eight years.
Sheknows exactly how long she suffered from the pain: four years and three months. It took years to diagnose her ailment, just two hours to fix it.
While she continues to recover from the dime-size hole and intrusion of endoscopic instruments into her skull, the vocal cord pain is a thing of the past.
"I’m pain-free, it’s gone," she said. "It disappeared immediately after surgery. I was sedated and when I woke up, Dr. Jimenez was right there. He kept asking me, ‘Does your mouth hurt? Is it gone? Is it gone?'"
Hathaway hopes her story will be an encouragement to others who suffer from the same condition, who look normal yet endure pain so unrelenting and severe that it causes suicidal thoughts.
"God gave me the strength, from the love of my children, to stay alive until I found Dr. Jimenez," she said. "Now I’m going to make a difference. I want to start saving lives of people with this disorder."
Learn more about minimally invasive endoscopic surgery.
[pexyoutube pex_attr_src="https://www.youtube.com/watch?v=Z7c29S-dhFc&feature=youtu.be"][/pexyoutube]

Neurosurgery’s history begins with a “Story”

Neurosurgery’s history in the Long School of Medicine dates back to the school’s infancy. The Division of Neurosurgery was founded in 1967 by Jim L. Story, M.D., at the Robert B. Green Hospital in downtown San Antonio. In 1974, the residency training program became fully accredited by the Accreditation Council for Graduate Medical Education (ACGME). Dr. Story trained nearly two dozen neurosurgery residents before his retirement in 1996.
In 2004, the Long School of Medicine recruited David F. Jimenez, M.D., FACS, (pictured above) from the University of Missouri. Since that time, Dr. Jimenez has built a Department of Neurosurgery that has 70 faculty, staff and residents and recently gained ACGME approval to expand to become one of the country’s largest neurosurgery residency programs. The department also obtained authorization to offer a prestigious spine fellowship.
In 2008, Department of Neurosurgery faculty agreed to staff the Baptist Health System’s Brain & Stroke Network, which provides neurosurgery support to stroke victims around the clock, 365 days a year. Prior to the network’s establishment, some stroke patients from Bexar County and the region were transferred to hospitals in other cities when care was not locally available.
Watch an interview of Dr. Story.
[pexyoutube pex_attr_src="https://www.youtube.com/watch?v=-wlqZEZJf5g&feature=youtu.be"][/pexyoutube]
Dr. Xin-Yun Lu: Mentor, mom, scientist
"Mentor," "mom," "scientist" and "game-changer" are fitting words to describe Xin-Yun Lu, M.D., Ph.D., associate professor of pharmacology in the School of Medicine at the Health Science Center. As a devoted mom, Dr. Lu attentively raises her children and steers them on a path toward success. Similarly, as a dedicated researcher, Dr. Lu is consistently raising up scientific discoveries that could pave the way to a novel class of medications for depression. One recent discovery even offers a solid clue as to why the risk of depression is doubled in persons with Type 2 diabetes.
Xin-Yun grew up in Northern China, where she attended medical school at Binzhou not far from Beijing. In 1992 after several years of study, she moved to the United States, where in a few years she completed her Ph.D. at Washington State University and a postdoctoral fellowship at the University of Michigan. Today Dr. Lu is one of the leading women scientists at the Health Science Center. Her novel studies of fat hormones’ role in depression – including the idea that these hormones could treat the disease without the metabolic side effects of current antidepressants – are highly cited by other scientists in journal articles worldwide.
"Fat secretes a lot of hormones, two of which are leptin and adiponectin," Dr. Lu says. "Our team has shed light on their role in mood disorders and their potential as antidepressant agents." In 2006 her lab reported that leptin, which regulates appetite, was decreased in rats that exhibited depression-like behaviors such as anhedonia (reduced pleasure seeking) and learned helplessness. The team’s findings led to more recent discoveries by other scientists that leptin is decreased in a broad spectrum of women with depression.
Another milestone came in 2012 when the lab published its discovery that levels of adiponectin, a circulating hormone that sensitizes the body to insulin, are lower in mice undergoing chronic social stress. When the team injected mice with adiponectin, this effect was reversed. This offers an intriguing connection between diabetes and depression. Current antidepressants raise the risk of obesity and Type 2 diabetes and do not help all depressed patients.
Dr. Lu is raising two daughters, Wendy, now 17, and Jenny, 11, with her husband, Wei Zhang, M.D., Ph.D., a third-year pathology resident in the Long School of Medicine. And even while overseeing a lab that includes four postdoctoral fellows, one Ph.D. student and one junior faculty member, Dr. Lu still finds time for her family’s activities. Since 2003 Dr. Lu has supervised at least 10 postdocs. She also has a lab and is a visiting professor at Binzhou Medical University, the institution that birthed her biomedical career.
Nicole Carrier, Ph.D., learned about Dr. Lu’s research while at the National Institutes of Health. Dr. Carrier is interested in why females are 2.5-times more prone than men to develop depression. "I came here to study gender differences in how leptin affects depression," Dr. Carrier said. "This was the only lab in the country doing this. The novelty is that this lab pioneered the whole idea of leptin in depression."
Jing Liu, Ph.D., instructor/research, said: "I joined Dr. Lu’s lab in 2006 and since then Dr. Lu has been a great mentor for me and a role model of a successful woman scientist. Her research has opened a whole new aspect of understanding mood and emotion regulation by hormones derived from adipocyte (fat). As a brilliant scientist, Dr. Lu’s enthusiasm and complete devotion to scientific research, together with her great wealth of knowledge, inspires and supports everyone in her group. As a respected mentor, she strongly encourages the development of both analytical and grant-obtaining skills, the two critical abilities for future scientific career development. It is exactly the fusion of her passion, charisma, intelligence and the exemplary style of her mentorship that makes me very confident about my future scientific career."