
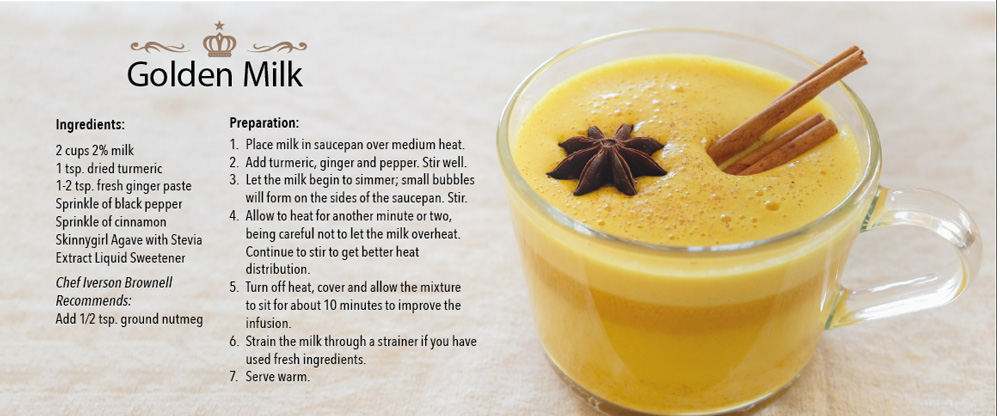
Spice it up
A little ginger, nutmeg, turmeric and cinnamon can go a long way toward improving health. A new cookbook with healthy recipes aims to help you live longer.
By Lety Laurel
Don’t just drink plain milk. Try adding turmeric, ginger, nutmeg, a little black pepper and a sprinkle of cinnamon. To shortbread cookies, mix in rosemary and ginger. Like trail mix? Try adding coriander, turmeric, ginger, cumin and cardamom.
These ingredients, all anti-inflammatories, may save your life.
Inflammation can be beneficial—it’s the body’s way of protecting itself in response to infection or injury, adding nourishment or boosting immunity. But if inflammation is chronic or unresolved, it can increase cancer risk.
In 2015, researchers at UT Health San Antonio decided to try out a theory. If breast cancer survivors adopted a diet high in anti-inflammatory ingredients such as ginger, turmeric, garlic, green tea and deep-sea fish, and low in inflammatory ingredients such as processed foods and sugars, red meat and fatty foods, they believed the risk of cancer recurrence would decrease.
More than 150 women participated in the study, called Rx for Better Breast Health, funded through Susan G. Komen. Over a year, they received cooking classes, led by local chef Iverson Brownell, counseling and biomarker assessments to test the effects.
It wasn’t long before participants began reporting significant changes in their health and the health of their family members. Blood pressure levels went down. Energy levels increased. Although this was not a weight-loss diet, the pounds began coming off. Participant Pamela Cresswell noticed an improvement in her lupus symptoms.
“Suddenly, I didn’t ache. I felt better, too,” she said.
Soon, the women were collecting and sharing recipes. Spices never before used became staples in their everyday cooking.
“The funny thing is that the stuff is so good. It tastes wonderful,” Cresswell said. “I found that I liked everything, and now I use everything they taught us.”
The women surprised themselves, said Dorothy Long Parma, M.D., M.P.H., an investigator on the study.
“This is not the way we’re used to eating,” she said. “Some of us have never heard of turmeric or know where to find it in the grocery store. I was very surprised to find how they embraced the ingredients they weren’t used to eating.”
 The study had another unexpected outcome. The women believed the recipes they discovered should be shared beyond their group of study participants. So a year after the study began, the women, guided by Chef Brownell, created The Rx Cookbook: Cancer-Fighting Recipes, Restaurants & Markets.
The study had another unexpected outcome. The women believed the recipes they discovered should be shared beyond their group of study participants. So a year after the study began, the women, guided by Chef Brownell, created The Rx Cookbook: Cancer-Fighting Recipes, Restaurants & Markets.
“We didn’t actually plan on doing a cookbook as part of the research protocol at the very beginning of the study, but it evolved because they were so interested,” Dr. Long Parma said. “It grew over time.”
The book features local fare such as barbecue rubs and chili con carne. There are salad recipes that are familiar: chicken Waldorf salad and avocado salad. There’s even a dessert section with spiced baked apples and cookies. All of them contain nontraditional ingredients in such subtle doses that they may not be detected—even by picky eaters.
“Someone was bragging to me about how they made cauliflower mashed potatoes and the kids couldn’t tell there wasn’t a single potato in the recipe,” Dr. Long Parma said. Ginger, a particularly strong spice, was a little more challenging to add in small doses.
“But someone had this idea of freezing it in ice cubes and sticking the cubes in their cooking to control the amount,” Dr. Long Parma said. “After that happened, people started making smoothies. That’s where the recipes started flying around.”
Because finding anti-inflammatory ingredients can be challenging, the cookbook also features a list of local stores that sell a range of spices, as well as restaurants that use the ingredients in their selections.
“We hope people can use this cookbook to help reverse the imbalance in our diets and prevent inflammatory disease,” said Amelie G. Ramirez, Dr.P.H., interim chair of the Department of Epidemiology and Biostatistics and director of the Institute for Health Promotion Research. She led the Rx for Better Breast Health Study, along with Michael Wargovich, Ph.D., and Rong Li, Ph.D., professors of molecular medicine.
Although study results are still being analyzed, the researchers do believe that fighting deadly diseases through diet is possible.
And, Dr. Long Parma added, “It tastes good, too. It really does.”
Watch a video recipe of sweet potato, carrot and turmeric soup here.


It's coming. Are we ready?
Summer in South Texas brings with it images of fishing at a nearby lake. Picnics in the park. Swimming at the pool or barbecuing to the sound of cicadas as night falls.
What can mar these picturesque scenes comes in the form of an insect about a quarter-inch long.
The World Health Organization estimates that more than 300 million illnesses are attributable to mosquitoes each year. Malaria alone accounted for 214 million in 2015, and killed 438,000 worldwide.
Then there’s West Nile. Chikungunya. Dengue. Yellow fever. And in 2016, a little-known virus spread by mosquitoes became an international pandemic: Zika.
Last year, the World Health Organization declared Zika a “public health emergency of international concern,” a classification that has only been given four times in the organization’s history. The announcement came after an outbreak of the virus in Brazil in 2015 and an accompanying surge in fetal microcephaly cases. Microcephaly is a neurological condition, usually the result of the brain developing abnormally in utero, in which an infant’s head is significantly smaller than the heads of other children. Severe cases often feature a backward-sloping forehead.
“The information from Brazil was really terrifying,” said Patrick S. Ramsey, M.D., M.S.P.H., professor of obstetrics and gynecology. “They went from 62 cases of microcephaly in the entire country to over 4,500 in one year. And that’s what raised all the flags.”
As summer turned into fall, the virus had spread to 61 countries worldwide. By February 2017, the U.S. had 4,753 known cases in 49 states, all acquired while traveling abroad. Then the virus hit the U.S. mosquito population, with local transmissions in Florida and South Texas.
Then, a stroke of luck. The weather cooled and mosquitoes tapered off.
“We were lucky, because we had a decent freeze and the mosquito population was thought to be largely out of the community at that point,” Dr. Ramsey said. “We did have the cases that were locally transmitted in Brownsville in December, but then the cold weather came in and everything was in a bit of a lull.”
But as temperatures once again rise in Texas, so does the risk of an onslaught. And this year is expected to bring a particularly hot and dry summer, exactly the kind of weather in which Aedes mosquitoes—the type that carry the virus—thrive.
“We’re getting ready for a reactivation of Zika this spring or summer,” Dr. Ramsey said. “We’ll probably have many more cases in Texas than we had last year.”
Already, there have been 10 confirmed cases of Zika in Texas in 2017. The Centers for Disease Control and Prevention is monitoring 250 more pregnant women who have laboratory evidence of Zika infection, and their infants.
In preparation for an increase in high-risk pregnancies linked to Zika, UT Health San Antonio physicians at the Medical Arts & Research Center, in collaboration with University Health System, are building a regional Zika Care Center to provide community and regional providers with ready access to diagnostic testing, surveillance and follow-up for patients exposed to the Zika virus in pregnancy.
“If we have an outbreak in San Antonio, I think there will be some form of mild panic, and we’ll have to deal with that,” Dr. Ramsey said. “We’re getting our clinic systems revved up to the point of having a Zika clinic so we can have all our resources in one spot.”

From unknown to pandemic
Zika made its debut in 1947 in a monkey in the Zika forest of Uganda. There were few human cases, so the virus raised little alarm.
Fast forward 60 years to 2007, when the first outbreak of the virus was recorded in Micronesia, in the Western Pacific Ocean. Within seven years, there were outbreaks throughout the Western Pacific and in Southeast Asia.
In 2015, the first case of Zika was recorded in the Americas. Within a year, it was an epidemic in Brazil.
“Some of the emerging infections are ones that we’re newly discovering, but many of them, like Zika, are those that have been around and it’s now just a new opportunity for them to spread,” said Jason Bowling, M.D., assistant professor of infectious diseases. “It’s interesting that, particularly over the last few years, we’re starting to see these emerging infections become more prominent.”
Zika is transmitted primarily by Aedes aegypti mosquitoes, distinguishable from other mosquitoes by their striped legs.
They live in tropical, subtropical and temperate areas, such as the southern U.S., Puerto Rico and the U.S. Virgin Islands. They live in populated areas because they prefer to feed on people.
“Mosquitoes in general are not good to people or other animals, for that matter,” said Dr. Bowling. “They cause a large amount of death and disease to humans and all other animals because of malaria and all other diseases they transmit. Malaria is probably the biggest one globally, but Zika is now on that list.”
The virus is closely related to the dengue and yellow fever viruses and lives in blood and seminal fluid, so a person infected with the virus can spread it sexually, and pregnant women can transmit the virus to their unborn babies.
About 80 percent of those infected are asymptomatic or have mild symptoms such as fever, rash, joint or muscle pain, conjunctivitis and headaches, although there has been a corresponding increase in Guillain-Barré syndrome in adults in areas affected by Zika. Those affected with the disorder, in which the body’s immune system attacks part of the peripheral nervous system, have weakness and abnormal sensations in the legs, arms and upper body. When severe, the person is almost totally paralyzed.
But in most cases, Zika goes unnoticed. For those who do experience symptoms, they last about a week, even though the virus can remain in bodily fluid for eight weeks in women, and up to six months in men.
And this presents the biggest challenge, Dr. Bowling said. Most people won’t know they’re infected and won’t take care to prevent transmission by using bug sprays with DEET to keep mosquitoes away or by using prophylactics during sex.
“One of the risks is that people like to travel, particularly young healthy people of reproductive age,” Dr. Bowling said. “So while in San Antonio we may not have Zika in our mosquito pools, we obviously have a lot of people who travel. We’re a military city. We have a young healthy population, and they don’t have to travel far to get to areas with Zika.”
And the toll the virus takes on unborn babies is devastating.
“When it hits you, it’s like a bolt of lightning that will ruin your kid’s life before it is even born,” said Sidney Atkinson, M.D., associate professor of pediatrics and division chief for child neurology, developmental pediatrics, and genetics and metabolic disorders.
No vaccine, no treatment
Unknowns are the biggest drivers of fear, Dr. Bowling said. And there is much that is still unknown about Zika.
“What are the risks to older children? What about kids playing in the backyard? Are they at risk? We don’t know,” Dr. Ramsey said. “Or what about a baby who is 2 months old and gets bitten by a mosquito that is carrying the Zika virus? What is the risk to that child? We just don’t know yet.”
But every new case brings new discoveries.
“Unfortunately, it takes numbers of people who are infected to see what will happen and get a better sense of this virus,” Dr. Bowling said. “But that’s not reassuring.”
Scientists are looking to Brazil and French Polynesia for answers.
“Some of the earliest data is from Brazil,” Dr. Ramsey said. “They had around 100 women with Zika who were pregnant when they were exposed to the virus. And of those women, only about 28 percent of them had any ultrasound findings that would suggest problems. Those were women who were definitely infected. Then of those, the babies with severe microcephaly were 19 percent. So that gives us some reassurance that even if you get infected, it’s not 100 percent [that the baby will be infected].”
In French Polynesia, located in the South Pacific, one out of every 100 Zika-infected mothers has a child with microcephaly.
“That one in 100 number is scary,” Dr. Atkinson said. “Depending on how widespread Zika becomes, it could be that a lot more local babies will be [infected than originally thought].”
To date, there have been 1,367 pregnancies in the U.S. with laboratory evidence of Zika virus infection. That includes those that ended in a live birth, miscarriage, stillbirth or termination, according to the CDC. Of the live births, 58 babies had birth defects. Seven pregnancies with birth defects were lost.
Probably the greatest risk to fetuses is in the first trimester, Dr. Ramsey said. The virus appears to attack the immature neurons in the fetal brain, which are abundant in the first months of pregnancy. This leads to congenital Zika syndrome, characterized by the presence of severe microcephaly where the skull has partially collapsed, decreased brain tissue with a specific pattern of brain damage, damage to the back of the eye, joints with limited range of motion and too much muscle tone restricting body movement soon after birth.
“Microcephaly is such a short word for what it does to your brain,” Dr. Atkinson said. “Microcephaly is really bad because it means the brain did not form. Think of all the things that we do that depend on the brain—eating, rolling over, breathing, all of those things are disordered in children with microcephaly. Some can have microcephaly and can have basic skills, but at the more severe end of the spectrum, kids never learn to sit up, never learn to roll over, never learn to crawl or walk, never learn to talk.
“Children often die in the first decade of life because the brain is so malformed and they can’t do anything. They can’t protect themselves in any way. That’s the kind of thing that we’re worried about with Zika.”
Before Zika entered the U.S., the number of babies born with microcephaly was small, two babies for every 10,000 live births. That translates to between 400 and 800 each year, and between two to five babies born in San Antonio with the disease. Even though Dr. Atkinson predicts only a slight increase, about 1 percent, in Zika cases locally, he said he’s bracing for the worst. He is part of an expert-action team at UT Health San Antonio assembled to manage children with congenital Zika syndrome.
“It’s not great frequency, it’s the severity that is the problem,” he said. “I think that there is going to be a rate of hurt children and it breaks my heart that it is going to happen, but it’s not going to be with such frequency that we’re going to have an epidemic like polio.”
Maternal-fetal medicine doctors at UT Health’s Women’s Health Center at the MARC specialize in high-risk pregnancies in partnership with University Hospital System. They now have an established Zika policy and standard procedures in place for screening for Zika, and implementation of testing strategies once there is a patient identified who may be at risk.
“We’re also educating the community,” Dr. Ramsey said. “We’re getting information out about what the risks are, the algorithm we’re using at University Hospital and here, and we’re sharing that with other hospital systems so they can implement something similar so we have better testing.”
Shrinking world, growing risk
Before Zika, there was Ebola. Before Ebola, there was West Nile. And don’t forget the H1N1 swine flu. Over the past few years, there have been a number of infectious diseases that have caused worldwide havoc. Health officials benefitted from that.
“Nobody saw Zika coming,” Dr. Ramsey said, but “we responded extremely briskly to Zika. Within two months of this starting to raise concerns, the CDC, the American College of Obstetrics and Gynecology, and the Society of Maternal Fetal Medicine all had consistent guidelines that were released. And we’re doing that at the local level, too.”
Dr. Ramsey has been working with those entities, as well as the Texas Department of State Health Services, to strengthen communication about Zika and perinatal risks to providers and patients. He’s working to improve access to Zika testing for obstetric providers and preparing new testing guidelines.
He’s also working closely with the CDC’s Zika response team to brace for a widespread outbreak in the state this summer.
“I think they’re preparing for the worst,” Dr. Ramsey said.
Students have also responded. Even as fall gave way to winter and the mosquito population died away for the season, students and faculty with the Center for Medical Humanities & Ethics began meeting with community members on San Antonio’s South Side in the country’s first Community Health Club. The program works to bring health education and behavioral changes to communities around the world. The club’s first subject: Zika.
Students also conducted a community needs assessment and shared local and regional information with obstetric providers and patients in Bexar County and surrounding areas. That student-led project will expand to the three largest obstetric delivery counties in South Texas: Cameron, Hidalgo and Nueces.
“I want to get out there and make sure the hospitals know how they should be approaching this, what the risks are and that we’re here to help,” Dr. Ramsey said.
In UT Health San Antonio labs, researchers Xiangzhi Meng, M.D., Ph.D., assistant professor of research, and Yan Xiang, Ph.D., associate professor, both in the Department of Microbiology, Immunology and Molecular Genetics, have made an infectious cDNA clone of Zika. This allowed them to create a Zika virus that expresses a green fluorescent protein so the researchers can easily monitor the infection of cells.
“This is an important and unique tool for us to use in studying the Zika virus,” Dr. Meng said. “It can also be used in screening for drugs against Zika virus.”
Meanwhile, scientists around the globe continue to work on a vaccine. While it typically takes a decade to develop a vaccine, researchers are pushing to have a Zika vaccine available by 2018. Already, several potential vaccines are undergoing clinical trials. Until a viable vaccine is found, approved and distributed, prevention and knowledge are the only defenses.
“The risk [of congenital Zika syndrome] is very small, but if it happens to you it’s absolutely devastating,” Dr. Atkinson said. “So I would caution people to be very thoughtful about mosquito bites and where you are going to be and when you are going to go outside when you are pregnant.”
The world is a smaller place now than it was decades ago, with travel becoming faster and easier, Dr. Bowling said. That has quickened the spread of disease, too.
“We are seeing diseases in one continent quickly popping up on another continent,” he said. “I think Ebola made it really hit home that things in Africa can come here, too. Africa is only a 16-hour plane flight away, and there are planes going there every day. We have to be cognizant of different infections and vector-born diseases all around the world.”
No one is immune to Zika, but that shouldn’t keep people from enjoying the warm days of summer and spring, he said. So go on that camping trip. Take a cruise to a tropical island. Go fishing at the lake.
“You don’t want to scare people—you want to empower them. And information is helpful for that,” Dr. Bowling said. “People are still going to travel and they should. We don’t want to paralyze people with fear, but they should all take precautions to protect themselves.”

The heart behind her science

Nicole Baganz was always interested in science, receiving her first microscope in second grade. It’s just that she wasn’t always that good at it, she said.
So she embraced the arts, and grew up playing the piano. She studied dance for 20 years. A teacher told her to forget her pursuit of the sciences and study English instead. That’s about the time she decided her future, and it was going to be in front of a microscope.
Years later, she’s embraced both passions in a journey that has taken her to the hospitals of China, the research labs of Vanderbilt, the rhythms of music and the depths of the human brain.
“I never saw my life taking this course,” she said. “The more we can experience in life, the more enriching our lives are and our communities are. Every single person we meet has a story to tell that you can learn from. If we stay in a bubble, we’re not going to learn all that we can and make ourselves better human beings. Life is an adventure.”
Growing up, though, Nicole was the reserved and safe one in her family. Her sister was the adventurer, the risk taker. But drug addiction and depression took their toll; her sister died of an overdose as Nicole was finishing her undergraduate degree in biology at the University of Wisconsin Eau Claire.
Nicole’s life veered sharply. She decided to move back home to be near her grieving family. While there, she studied massage therapy.
“I wanted to work with people instead of being in a lab, which is funny considering where I am now,” she said.
Then a flier from Midwest College of Oriental Medicine appeared on her desk and piqued her interest. It advertised a master’s degree in traditional Chinese medicine.
“So I taught anatomy and physiology in two different massage therapy schools and a nursing college to put myself through school, and that’s when I realized I really loved teaching physiology and I was good at it,” she said.
After getting her master’s degree in traditional Chinese medicine, becoming nationally certified in acupuncture and Oriental medicine and traveling to China for an internship, she decided to pursue a Ph.D. in physiology, with an emphasis in neuroscience at UT Health San Antonio. She wanted to unlock the mysteries of the brain that lead to the mood disorders that devastated her sister.
“With my sister’s story, I specifically was interested in neuroscience,” she said. “They accepted me not as a Ph.D. student, but as a master’s student because my background was very nontraditional.”
 By the end of her first semester, she had proven her high school teacher wrong. Her grades put her at the top of her class, and she was moved into the Ph.D. program. Hers was the inaugural class in the neuroscience program. She graduated in 2009 as the highest-ranking student in her class, receiving the Armand J. Guarino Award for Academic Excellence in Doctoral Studies.
By the end of her first semester, she had proven her high school teacher wrong. Her grades put her at the top of her class, and she was moved into the Ph.D. program. Hers was the inaugural class in the neuroscience program. She graduated in 2009 as the highest-ranking student in her class, receiving the Armand J. Guarino Award for Academic Excellence in Doctoral Studies.
After completing a year as a postdoctoral fellow at UT Health San Antonio, she moved to Vanderbilt University Medical Center in Nashville, Tennessee, where she worked as a postdoc and later became a research instructor. It was in Music City—appropriately—that her love for the arts professionally collided with her love of science.
She began studying how music affects the brain, and organized Nashville’s first Music and Mind seminar that brought together musicians and scientists on one stage. Her attempts to bring neuroscience into the mainstream didn’t stop there. She organized walks to support the National Alliance on Mental Illness, and spoke to groups throughout the city about the brain. She shared her family’s story about mental illness and her personal quest to uncover the biology behind it.
“When I wasn’t doing experiments in the lab, I was talking to people outside of the lab about the brain. I thought we shouldn’t be afraid to tell our stories anymore,” she said. “The more I went out to the community and started talking, the more they would talk back and they started caring about the brain. And I was shocked at how little people knew.”
Her goal: Erase the stigma of depression and other mood disorders by showing there’s a biological reason for the behavioral symptoms. To do that, she said, requires breaching the walls of academia.
“We have a responsibility to our community to share the information that we know and keep our communities healthy and knowledgeable,” she said.
But so much of science is black and white, with no room for emotion, her critics said.
“I have had scientists tell me that I shouldn’t be doing my science because I have a reason to do it, and I thought that was the weirdest logic I have ever heard,” she said. “They said I shouldn’t be studying mood disorders because of my sister. But what is going to keep me going every day? I need to do it. So I think it’s a good thing to have heart behind your science.”
She took that passion with her to Florida Atlantic University, where she now works as a research assistant professor in biomedical science. She’s studying how changes in the immune system can have a depressive effect on mood. She is also helping create the university’s first Brain Institute, a research facility that will offer master’s and Ph.D. programs in neuroscience. As the director of community engagement and programming for the Brain Institute, she will ensure community outreach also will play an important role.
“Neuroscience is growing by orders of magnitude every day, and I’m excited that hopefully we will totally erase the stigma of mental illness soon,” she said.
The arts and sciences have blended to make Nicole a better scientist, she said. She thinks differently, asks different questions. Her nontraditional path has added new dimensions to her work.
“When my experiments work, I dance in the lab,” she said.
Sometimes she imagines what her life would be like if she had become a dancer instead of a scientist.
“But then when the experiments work, and we find another potential target for treatments for mental illness,” she said, “I am reminded why I chose the science road.”

Healing starts here
Rosanne Fohn contributed to this story.
In ancient times, medical advances were made through a mixture of experimentation, observation, trial and error. By those standards, clinical trials have been going on for thousands of years.
But today’s trials, heavily regulated by the Food and Drug Administration, are a far cry from the methods of discovery made by early civilizations. Now, long before humans become involved, there are decades spent in laboratories across the world, basic scientists poring over data sets, seeking answers, creating hypotheses. Theories are tested on cell cultures, then fruit flies. Small animal studies then follow.
Theories are strengthened. Some are disproven.
A few make it through to clinical trials.
This is where the path to healing begins.
***
Mona Lisa Mejia’s life changed in April 2015. She began having severe headaches—what she believed were bad migraines. There was crushing pain. Nausea. Weakness.
What was believed to be a sinus infection was eventually diagnosed as Stage 4 non-small cell lung cancer that had spread to her brain.
Her case was somewhat unique. While non-small cell lung cancer is the leading cause of cancer-related deaths worldwide, about 15 percent of patients also have a genetic mutation of a critical protein. That protein, called epidermal growth factor receptor, lies on the surface of cells and causes normal cells to grow and divide. In these rare cases, too much of the protein fuels rapid growth of tumors throughout the body.
She immediately began radiation therapy to shrink her brain tumors. For her lung cancer, she turned to a clinical trial.
Life-changing results
The university has offered clinical trials almost since the day it opened in 1968. Clinical trials are research studies that depend on human volunteers to explore whether a medical strategy, treatment or device is safe and effective for humans.
Clinical trials may involve treatments under development by pharmaceutical or biotechnology companies, or by independent researchers. Some test new therapies, while other trials test new combinations of already available treatments.
“At any one time at [UT Health San Antonio], we have about 1,500 research studies that involve humans,” said Joseph Schmelz, Ph.D., assistant vice president for research administration. Not all of these research studies end up in clinical trials, however. Many depend on human volunteers simply for observation.
“If we drill down, probably half of those are clinical trials where we are actually testing and looking for ways to deliver health care,” he said.
On average, about 160 new clinical trials are started here each year. Studies can range from endodontics and respiratory care to diabetes treatments and cancer therapies. The majority are cancer trials, mirroring the national average of about 30-40 percent of all trials.
“As an academic health institution, we have faculty who are doing research in all areas. You’re not going to get that anywhere else in San Antonio,” Dr. Schmelz said. “There are plenty of great physicians in the city, but what is unique about [UT Health San Antonio] is that it’s where clinicians and scientists and physician scientists come together and collaborate. That’s what it takes to do science.”
And that science can have life-changing results.
In 2013, a study on finasteride, a drug used to treat enlarged prostate and male pattern baldness, was called one of the most significant practice-changing discoveries of the year. It took researchers from the Cancer Therapy & Research Center (CTRC) more than a decade to conduct the first trial, then they continued with dozens more that followed 19,000 men over many more years. The result: a new prevention drug for prostate cancer that reduces a man’s risk of prostate cancer by almost a third.
Around the same time, the first clinical study to prove that children’s oral stem cells could regenerate their teeth was conducted by researchers in the School of Dentistry. The discovery led to the definition of a new term in the field: regenerative endodontics, and a new treatment offering for children facing the prospect of total tooth loss or a root canal.
And just last year, a CTRC patient became the first person to have radioactive nanoparticles inserted by a catheter into a tumor of the deadliest form of brain cancer, glioblastoma, which kills two-thirds of patients within five years. The experimental gene therapy was found to nearly double the overall survival of patients with a recurrence of the cancer.
Breakthrough studies are continuously underway: The first pharmaceutical intervention shown to extend the lifespan of middle-aged mice, rapamycin, was first proposed by university researchers as an intervention for aging and has been used in cell and animal studies ever since. The first human clinical trial began in 2013 and is ongoing.
“You think of the investment that goes into the science that it takes to create that kind of treatment, it’s almost immeasurable,” Dr. Schmelz said. “You think of all the postdocs and all the people that work in those labs and all the experiments they do over sometimes 25 or more years, to get to this point and build upon those ideas, it’s all to improve health care.”
[bgsection pex_attr_title="Step 1" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="16cc16" pex_attr_textcolor="000000" pex_attr_height=""]
Right now, researchers are trying to regrow salivary gland cells in a micro-environment in the hopes that someday they can transfer them into patients.
Once salivary glands are damaged, the effects are permanent. Tissue engineering could help millions in the U.S. with dry mouth due to Sjögren’s syndrome, as well as radiation for head and neck cancer.
[/bgsection]
Searching for help
Mona Lisa Mejia’s diagnosis of non-small cell lung cancer was a blow to her family. They were still recovering from the death of her 18-month-old daughter to sarcoma, a rare cancer that grows in the body’s connective tissue. And with the double whammy of the genetic mutation in her own body, Mejia’s treatment options required a unique solution.
Her doctors turned to a clinical trial to compare two treatments for the specific type of cancer she has.
She began treatment June 1, 2015, receiving afatinib, an oral medication. Another group of patients received intravenously a combination of that drug and cetuximab, a common chemotherapy treatment.
Through the trial, researchers are trying to determine which treatment option is the best. Animal studies showed a combination of the drugs worked better than either one alone.
This June, a year after her first treatment, Mejia was given good news: her tumors have shrunk and are stable.
[bgsection pex_attr_title="Step 2" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="16cc16" pex_attr_textcolor="000000" pex_attr_height=""]

Right now, scientists are using fruit flies to explore ways to prevent the earliest triggers of Alzheimer’s disease.
Fruit flies affected by Alzheimer’s have tunnel-like features in the lamin, a mesh-like skeleton that protects brain cells’ control center. This shows lamin dysfunction can cause the death of brain cells, something that appears to be specific to Alzheimer’s.
[/bgsection]
A complicated process
Before a new treatment can be tested in people, it must first go through a rigorous discovery process in research labs. Possible side effects are evaluated through small animal testing, carefully regulated by the university’s Institutional Animal Care and Use Committee to ensure the research is performed in an ethical and humane manner. If there is success in animals, the next step is often human clinical trials. Before getting approval to move on to clinical trials, investigators must write detailed plans on why they are conducting the study and how it will be administered. What are they trying to prove? What is their primary end point? What is the time frame? How will data be gathered?
Everything is carefully documented. Federal guidelines must be followed to the letter.
It takes very little for this process to get tangled up, and for researchers to have to begin again. Some have to entirely scrap their projects.
“It’s really complicated,” said Bob Clark, M.D., MACP, assistant vice president for clinical research. “There are so many things that have to happen along the way, and they have to happen right and they are mostly in serial array so that if this one over here gets messed up, you don’t get to these other ones until much later, maybe.”
Then the proposal must go through the university’s Institutional Review Board, which evaluates whether the study is ethical and volunteers are adequately protected.
“The closer they get to humans and the closer human research gets to clinical trials, the more regulations and oversight is placed upon the research,” Dr. Schmelz said. “It’s a burden in that it is additional work and effort, but it has to be done.”
Many proposals never clear this stage. Nationally, only one out of every 1,000 drug compounds in preclinical testing is promising enough to continue to the investigational new drug application process, according to the Department of Health and Human Services.
For those that do, they may face another decade or longer in clinical trials.
[bgsection pex_attr_title="Step 3" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="16cc16" pex_attr_textcolor="000000" pex_attr_height=""]
 Right now, scientists are searching for the root cause of Parkinson’s disease so that someday there will be a treatment.
Right now, scientists are searching for the root cause of Parkinson’s disease so that someday there will be a treatment.
Small animals afflicted with the disease are revealing a timeline of decline as the disease kills dopamine neurons, leading to debilitating movement deficits. Scientists hope understanding the disease’s progression could lead to a drug that will stop it and lengthen time patients have to lead healthy, productive lives.
[/bgsection]
Experiment, control, test
Ancient medicine that depended on observation and anecdotal evidence of successes and failures led to some key advancements in health care. Advancements in technology, data gathering and documentation, and lessons learned from global drug disasters led to the creation of the controlled and extensive therapeutic trials of today.
“You can’t even do a clinical trial until the FDA has blessed it,” Dr. Clark said. “There’s an additional level of assurance for volunteers that it is a legitimate and safe thing to do.”
Today’s clinical trials program is divided into phases, with phase 1 being the first time a new drug or device will be tried in a small number of people. It screens for safety, dosage ranges and side effects. Phase 2 includes a larger number of volunteers and tests effectiveness and safety. Phase 3, which involves several hundred to several thousand patients, confirms effectiveness and compares the investigational therapy to standard treatments already in use. Side effects are monitored and information collected to ensure the treatment will be used safely.
A treatment will only pass through to the next phase if it has been found safe and effective.
Phase 3 is typically the final phase before the therapy becomes available in the marketplace. Occasionally, a trial will enter phase 4, but this is largely reserved for therapies already approved by the FDA and being proposed for a new use.
“It is with this idea of rigorously testing ways that deliver health care in a scientific manner that we have the ability to decide whether the changes that we want to make really do result in improvements in health care,” Dr. Schmelz said. “Clinical trials are very much this idea of experimentation and controlling all of the variables and testing hypotheses.”
The rigor comes at a hefty price: Before a drug clears all phases to make it on the pharmacy shelf, the Department of Health and Human Services reports, it will cost anywhere from $44 million to more than $115 million. Dr. Clark said the reality is much higher—with scholarly articles estimating the cost at around $1 billion per drug.
“It is extremely expensive,” Dr. Schmelz said. Studies that originate with university investigators start out small, but as a therapy shows promise, it must be tested at multiple sites.
“Eventually they have to expand to multicenter clinical trials,” Dr. Schmelz said. “So that means you are going to have to migrate the research to other institutions and you are going to have to get other people at those institutions to run the trial for you. And in order to do that, it takes quite a bit of infrastructure.”
Funding comes from the federal government, private industry, medical institutions and foundations.
Finding participants
Even with the creation of online clinical trial databases that pair volunteers with investigators, many trials struggle to get enough participants for a legitimate study. Only about 3 percent of cancer patients enter clinical trials, according to the National Cancer Institute, and the reasons range from fear of a reduced quality of life to the inconvenience of participation. Nearly half of all cancer clinical trials nationally fail to enroll enough patients and can’t be completed.
Mona Lisa Mejia viewed her participation in her clinical trial with hope, even as she struggled with side effects from her cancer treatment. At the beginning, diarrhea and fatigue were constant battles until her body adjusted to the medication.
But being in the trial gave her purpose.
“My kids are worried about me, but we continue to have faith in God,” she said. “Our faith has gotten us through all of this and without it I would have lost hope. I prayed and he answered. He sent all of these angels to help me. I am just so grateful.”
For health or science?
Not every clinical trial works the way the researchers hypothesize. Patients for whom standard therapies don’t work hope for a miracle cure. Yet some may get no benefit.
If there is a benefit, but the study hasn’t yet cleared phase 3 and received FDA approval, the therapy will no longer be available for participants once their trial is complete. And there is never a guarantee that the FDA will approve the new therapy for use in people.
“We have an extensive informed consent process where we try to make all participants understand the limitations of their own personal benefit,” Dr. Schmelz said. “Really, the benefit is to the knowledge we will gain in the future, and I think most people are willing to give of their time and effort to help in science.”
Many participants realize that greater benefit when they enroll, Dr. Clark said.
“Partly they are hoping they might get some personal benefit, but I think many of them have a very broad perspective on it and a sense that it is something they’re doing for societal benefits,” he said. “They want to make a contribution.
“The trial may not cure whatever it is they have, but because of their involvement, physician scientists will learn something that will help future generations of people.”
[bgsection pex_attr_title="Step 4" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="16cc16" pex_attr_textcolor="" pex_attr_height=""]
 Right now, people of all ages are participating in clinical trials in the hopes of finding new therapies to eradicate the world’s deadliest diseases.
Right now, people of all ages are participating in clinical trials in the hopes of finding new therapies to eradicate the world’s deadliest diseases.
At any one time, the university has 1,500 ongoing research studies that involve humans. About 160 clinical trials are begun each year and can range from endodontics and respiratory care to diabetes treatments and cancer therapies.
[/bgsection]
Change agent
As a trauma and critical care Army nurse, Kimberly Smith served around the world, caring for the most critical of patients in the most dire of circumstances.
After nearly three decades, she’s serving in a new capacity: change agent.
Dr. Smith retired from the military and enrolled in the School of Nursing’s doctor of nursing practice program. She graduated in 2015.
“Over 28 years in health care, it’s the central focus that we all strive for to keep your patients safe, to advocate for them, to heal them and comfort them,” she said. “In trauma and critical care, you train teams to focus on the object of saving a patient’s life and you do that through different processes. Those processes that we use in health care all translate into patient safety, performance improvement and doing the best for the most.
“With the D.N.P., you have more of an opportunity to perform on a bigger scale to affect more lives, to affect more processes throughout the big system instead of a small team, a small system.”
The School of Nursing’s D.N.P. program, created in 2010 and accredited in 2012, is a seven-semester doctoral program designed to teach students how to identify a health care practice gap and use the best evidence to change it. Before graduating, students must identify a problem within the health care system and create, implement and evaluate a solution. It’s a project that spans years, and culminates with a presentation to area health care leaders.
Dr. Smith’s project focused on palliative care. She developed a business case model to implement a palliative care program at Brooke Army Medical Center (BAMC), where she worked during the first half of her degree program as a quality director before she decided to focus full-time on her education.
Palliative care focuses on improving the quality of life of those who have chronic disease and get sicker over time. While it’s an emerging health care field throughout the nation, few military hospitals had adopted any formal palliative care programs, she said.
Working with a team of clinicians at BAMC, she created a proposal that explored successful business models of palliative care programs, demonstrated potential cost savings and showed how it could improve patients’ lives.
“It was a multipronged approach to capturing the hearts and the minds of the leadership through lots of discussion and stakeholder meetings and the pure raw numbers of potential cost savings through the care of really chronically ill patients,” she said.
Not only did the military hospital administrators agree, but they also decided to fund the program and create seven full-time positions. The program began in December, and although it’s too early to tell whether it will yield positive results, Dr. Smith said she has no doubts about its impact.
“The evidence would show that it’s going to be dramatic,” she said.
Dr. Smith is now the vice president of clinical outcomes at Methodist and Methodist Children’s Hospital. In that role, she and her team are responsible for everything related to quality health care and patient safety, from patient flow to performance improvement on a small and large scale.
“It feels good to be able to implement change and be able to make improvements,” she said.
Since 1999, when the first D.N.P. program was created in Tennessee, more than 11,500 students have received D.N.P. degrees nationwide. It’s growing in demand, said Carole White, Ph.D., professor in the School of Nursing, because of the need for expertise in translating evidence into practice to standardize and improve the quality and cost of health care.
“Patient care is challenging as people live longer and have more chronic conditions that are more complex to care for, and we need to be sure we’re treating them with the best evidence,” she said. “We need to have people who can assess that evidence and bring it to practice, not only at the patient level, but at a system and population level.”
Students identify a practice gap and gather the evidence they need to implement change. They learn how to translate that knowledge into practice.
“They gain confidence in leading change,” Dr. White said. “D.N.P. graduates leave this program prepared at the highest level of nursing practice.”
Dr. Smith said her work today isn’t very different from the work she did as an Army nurse. The vernacular may be different, and the style of dress, she laughs, but the mission is the same.
“The work is still centered around the best health care that we can give to our customers, the safest health care we can give—measuring processes to do better and to perform better and to get people engaged more, not just with one patient but in a big system.
“I’m very proud of the work I have done.”

Out of the dark
Related story:
A difficult path
In Lisa Sanchez’s darkest days, she hid her family behind closed window blinds. She avoided friends and family.
She was embarrassed by the mental illness that caused her preteen son to uncontrollably shout out obscenities. Embarrassed when that son was treated poorly at grocery stores, church and school.
She was embarrassed that she didn’t know that bipolar disorder ravaged her daughter, leading to alcohol and drug abuse when the girl was in middle school. That the same daughter, her oldest, the one she always called “the strong one,” would wake up from a drunken stupor on the side of the road, so drunk she couldn’t get home. She was embarrassed that she never knew that daughter had a plan to kill herself until it was almost too late.
She’s not embarrassed anymore.
When Lisa talks of her three children, all of whom battled decades of mental illness, she cries, the pinwheel medallion that she wears around her neck catching the sun as she wipes away her tears.
“I’m happy. It’s a happy sadness that we made it,” she clarifies quickly.
They’re tears of relief. And pride.
“I’m blessed. God has blessed me with three children with mental illness. And we made it,” she said. “There’s light now.”
 Jacob Sanchez was just 4 years old when his mother first noticed something was different about him. He made it through four days of pre-kinder before she got the call saying he wasn’t ready for school. He screamed continuously. He needed to be carried by a staff member all day long. He was disruptive.
Jacob Sanchez was just 4 years old when his mother first noticed something was different about him. He made it through four days of pre-kinder before she got the call saying he wasn’t ready for school. He screamed continuously. He needed to be carried by a staff member all day long. He was disruptive.
Once he began staying with his grandmother, Lisa began noticing other things. The constant throat clearing. The repetitive motions that started at his face: first touching one cheek, then the other, before going to his chin. Beginning again. Increasing in frequency and speed as he grew agitated, nervous or excited. Then the barking began. Spitting. Whistling. Shouting.
Jacob was diagnosed with Tourette Syndrome, a neurological disorder characterized by motor and vocal tics, sometimes obscenities. Then came the potentially crippling triad that so often develops with Tourette: obsessive compulsive disorder, anxiety and depression.
By the time he was in middle school, he had been admitted to Clarity Child Guidance Center for emergency inpatient care twice, and had two intensive partial admissions. After two failed attempts at high school, he was withdrawn and homeschooled.
Those years were marked by constant fits of screaming and crying. It seemed endless, and for Jacob’s two sisters, it was unbearable.
One sister turned to drugs and alcohol. The other began displaying signs of obsessive compulsive behavior in elementary school.
“I was so overwhelmed with Jacob that I never picked up on it,” their mother said. “‘Dear God,’ I remember thinking, ‘How did it get to this?’”
A nation in crisis
 They call it a crisis. San Antonio, along with the rest of the country, is facing an epidemic.
They call it a crisis. San Antonio, along with the rest of the country, is facing an epidemic.
Across the country, one in five children has a mental illness. In Bexar County, that translates to 80,000 kids who are struggling with behavioral, emotional or mental illness.
Lisa had three in her small family. She never saw it coming. There was no family history of mental illness, no substance abuse problems. She, like many parents, was unaware of the prevalence of mental illness in children.
“If one in five kids in Bexar County had leukemia or some kind of cancer, we’d be having bake sales, and doctors and researchers would be working diligently to find cures,” she said. “But we have one in five kids who could potentially end up suicidal or in jail or dropping out of school or using drugs and alcohol, but the concern is not there.
“There is a stigma about mental illness, and that has led to a lack of resources.”
Nationally, there’s a “severe shortage” of practicing child and adolescent psychiatrists, according to the American Academy of Child and Adolescent Psychiatry. In Texas, there are eight psychiatrists for every 100,000 children.
“There is a huge need,” said Rene Olvera, M.D., M.P.H., division chief of child and adolescent psychiatry at the Health Science Center and outpatient medical director of Clarity Child Guidance Center, where the university’s child and adolescent psychiatry program is housed.
About 5 percent of medical students nationwide continue fellowships in child psychiatry. At the university, that number hovers around 4 percent, with the program capped to allow four fellows a year.
Before they leave medical residency, child and adolescent psychiatry fellows spend months in mandatory rotations at Clarity, as well as the San Antonio State Hospital, Bexar County Juvenile Detention Center and the Cyndi Taylor Krier Juvenile Correctional Treatment Center. They also train at area schools, an emergency shelter and neurology clinic, and offer pediatric consultations for University Health System.
“What we’ve tried to do is create an environment that allows our residents to see a full breadth of child psychiatry. And at the same time, we’re filling that gap for our community,” Dr. Olvera said.
 Mental illness can start as early as when a toddler takes its first steps. The most common illnesses are attention deficit hyperactivity disorder, depression, bipolar disorder and anxiety. Suicide is the second leading cause of death in children in Texas, and the third nationwide.
Mental illness can start as early as when a toddler takes its first steps. The most common illnesses are attention deficit hyperactivity disorder, depression, bipolar disorder and anxiety. Suicide is the second leading cause of death in children in Texas, and the third nationwide.
“I think society forgets or they don’t like to think about the fact that kids do kill themselves,” said Brigitte Bailey, M.D., training director of child and adolescent psychiatry.
But every appointment is an opportunity to save a life, said William Lee, M.D., a child and adolescent psychiatry fellow at the Health Science Center. In medical school, he decided to change his specialty from pediatrics to child psychiatry when he realized his favorite part of a patient appointment was asking how that patient was doing, how school was going, how things were at home—the questions that a physician doesn’t have much time to explore, but that he felt were the most critical.
“To hear a child articulate their problems to you and what they are struggling with, I think that is a very powerful moment,” he said. “When we think about childhood, it’s all the innocence, the fun, the play. If they cry, we think we can give them some ice cream and they’ll feel better. But that’s not always the case. And to be able to have someone sit across from you and tell you that they’re really struggling, they can be 8 or 9 years old, but their problems are real. That’s a real moment.”
It’s not sad, he said, though the circumstances that bring a child to the point of needing help often are.
“What I feel is hope,” he said. “When a child comes to you for help, you have the opportunity to make a difference for the rest of their lives. You have the chance to change their trajectory. That is something that is both a very powerful responsibility and an important responsibility.”
Lisa spent years visiting different neurologists, running every kind of medical test to determine the cause of Jacob’s muscle and vocal spasms. She didn’t feel hope until she arrived at Clarity. Like the name promises, a sense of clarity overcame her, she said.
“We shouldn’t be so stigmatized and so worried about what people are going to think and get the help our children need,” she said. “Just like you worry about your child getting the flu or meningitis, worry about your child having mental health issues. And don’t be afraid to question doctors if you feel something is wrong with your child and no one is listening. Because no one knows better than you.
“I waited too long.”
It wasn’t that Lisa didn’t know there was a problem—she was working so hard to fix it herself. She thought if she was a better parent, the problems would go away.
“I just didn’t think I was doing it right,” she said.
The night Jacob was admitted to Clarity was the first night in years that Lisa got a full night’s sleep. She was at peace.
With new eyes
Lisa’s home is a different place these days. It’s been a decade since her darkest days of hiding. Mental illness doesn’t go away, but it can be managed. Jacob, now 22, still spits. He still barks and has other noticeable motor tics. But he also has a full-time job at a local hospital as a transport tech in the emergency room. He goes to movie theaters again, something he stopped doing at the height of his illness. Years of psychotherapy, behavioral interventions, medications and electroconvulsive therapy got him this far.
Through psychiatric care, his oldest sister learned how to manage her bipolar disorder. She no longer self-medicates with drugs and alcohol. She now travels around the world on mission trips and hopes to someday join the Peace Corps. She’s 24. Their younger sister is 19, and has devoted her life to helping fellow students with special needs. Her hope is to become a psychiatric nurse practitioner.
They’ve all been touched by mental illness, their futures shaped by it. Jacob says he’s blessed with it.
Just before the Easter holiday, Lisa saw her family with new eyes. Her daughters were home for the holiday. Jacob had taken time off from work. They all sat together on the oversized sectional in their living room, the evening light filtering through their open window blinds. There was laughter as they swapped stories. And she thought, it’s taken us a long time to get here, but finally we have arrived.
[bgsection pex_attr_title="A difficult path " pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-dark-bg" pex_attr_bgcolor="f5f3e4" pex_attr_image="" pex_attr_imageopacity="0.5" pex_attr_bgimagestyle="static" pex_attr_titlecolor="000000" pex_attr_textcolor="000000" pex_attr_height=""]
 Becoming a child and adolescent psychiatrist isn’t fast and it isn’t easy. Following medical school is a grueling five-year residency program, with three years spent in adult psychiatry and a two-year child and adolescent psychiatry fellowship. That’s the same number of years required to become a general surgeon, said Brigitte Bailey, M.D., training director of child and adolescent psychiatry.
Becoming a child and adolescent psychiatrist isn’t fast and it isn’t easy. Following medical school is a grueling five-year residency program, with three years spent in adult psychiatry and a two-year child and adolescent psychiatry fellowship. That’s the same number of years required to become a general surgeon, said Brigitte Bailey, M.D., training director of child and adolescent psychiatry.
“There has always been a shortage of child psychiatrists,” said Dr. Bailey. “It’s a lengthy road.”Once they’re out of school, they face other challenges: Insurance reimbursement rates are notoriously low. Unless you work in private practice, it isn’t lucrative. And it’s a lot of work.“You need to wake up loving your field of medicine because you’re going to spend long hours and you’re going to invest a lot to do it,” Dr. Bailey said. “We need that idealistic spirit to come into this because we want to work with families and do good work.”
The average wait time for a child to see a psychiatrist in the city is more than three months. Community assessments estimate San Antonio is 45 beds short on any given day.
Still, the city is better off than other areas of the country, said Dr. Bailey.
“Our program here has an overwhelming impact,” she said. “We’re quiet, but we’re everywhere. And our trainees are everywhere in San Antonio.”
Those trainees tend to stay in the area after residency, helping keep the psychiatrist-to-child ratio lower.
“Not only do we train them, but because we’re in the community, that commitment continues long after they leave here,” said Rene Olvera, M.D., M.P.H., division chief of child and adolescent psychiatry at the Health Science Center and outpatient medical director of Clarity Child Guidance Center. In April, Clarity opened an outpatient therapy facility that now houses the Health Science Center’s child and adolescent psychiatry program.
Dr. Olvera estimates that 90 percent of Clarity’s staff was trained at the Health Science Center.
“It’s a dual function while they’re here, as our fellows are learning while providing patient care,” he said. “The beauty is that the payoff to the community goes on for decades.”
[/bgsection]

A second calling

After losing both of his legs above the knee in an IED blast during his deployment to Afghanistan in 2005, U.S. Army Special Forces medic Roland Paquette received a Purple Heart, underwent rehabilitation and took a government job.
But the same desire to serve that drew Paquette to join the military after 9/11 is what pulled him back to patient care. He enrolled at the Health Science Center and earned his master of physician assistant studies degree in 2012. Paquette is now a physician assistant in the Department of Emergency Medicine at the Health Science Center and adjunct faculty in the Department of Physician Assistant Studies.
“I had felt that kind of bug before where I just needed to go do something,” he said. “I was feeling the same thing about getting back to patient care and doing medicine.”
Paquette, 37, said his own experience shapes the care he gives patients, but he is careful to keep the focus on them.
“At least once a day on a shift, when I see a patient who is experiencing pain or has experienced an injury or whose family seems more stressed out than others, I think I can empathize with that,” Paquette said.
His experience allows him to foster trust with patients that can be tough to build when medical professionals are sometimes viewed as adversaries.
“I’m not just somebody in a white coat on the other side of things,” Paquette said.
If people ask about his prosthetics, Paquette will share his story, when appropriate.
“What I don’t want to do is make someone feel like I’m minimizing what they are going through,” he said.
Sometimes patients or their families with whom he hasn’t shared any of his background will ask if he injured his back—something he takes as a compliment.
“I take it as a sign of success,” he said. “I don’t have any legs and this person thinks I may have hurt my back.”
His experience in physical and occupational rehabilitation enables him to give patients a sense of what to expect in their own journey. It is hard to accept limits on physical ability, and there are low points along the way, he said. What made a difference for him was having clear goals for his rehabilitation. He urges patients to focus on the “why” of recovery.
“It is hard, painful and very frustrating,” he said. “If you can, put it into a better context: Why is it you want to rehab? Why do you want this wound to get better? Why do you want to get more mobile?”
Aside from his clinical work, the father of three also trains first responders through a company he started last year. He also mentors soldiers through the nonprofit Green Beret Foundation, which his wife, Jennifer, heads as executive director. Recently, he served as the principal investigator on a study comparing the effectiveness of tourniquets to hemorrhaging clamps in massive extremity hemorrhages.
“I feel really satisfied with what I’m doing,” Paquette said. “I think you just keep swimming upstream and that’s what I’m doing. You just keep trying to work with what you’ve got.”

No ordinary lesson

They treated victims of abuse, and people who had lost everything after some unforeseen, devastating crisis. They treated prostitutes and drug users who measure time by the number of days since their last fix. They treated people living on the streets who used every last cent they had on a meal, not a toothbrush.
They were at times met with anger and impatience, were sometimes yelled at and cursed, but were also blessed and thanked.
They treated, they listened. They nervously confronted their own stereotypes. And now, they say, they feel ready to become dentists.
All fourth-year dental students must complete more than 31 days of clinical rotations in San Antonio and South Texas before graduating. Yet there’s one clinic that is met with both dread and anticipation. The mandatory rotation is at San Antonio Christian Dental Clinic at Haven for Hope, which provides free dental care for homeless and underserved adults and gives the students a unique patient pool with challenges rarely, if ever, experienced by students, said Vidal Balderas, D.D.S., M.P.H., assistant professor of comprehensive dentistry.
“Most students have never had the opportunity to be a part of cases where they’re exposed to [post-traumatic stress disorder], addiction, bipolar disorders—sometimes all in the same patient,” he said. “Our primary goal of the experience at San Antonio Christian Dental Clinic is to expose our students to patients whose lives have been compromised. It’s almost assured that at least one of those experiences with the patients we deal with there will be heart-wrenching. You can’t help it. When you’re homeless, something devastating put you on the streets.”
Haven for Hope has served more than 6,870 residents since it opened in 2010. In that time, they have accounted for 2,800 visits to San Antonio Christian Dental Clinic.
“For many, the nature of poverty and homelessness becomes tangible at San Antonio Christian Dental Clinic,” said Gloria Canseco, executive director of the clinic. “Students come face-to-face with profound cases of patients who have suffered from domestic violence, substance abuse, mental health, abandonment and other severe obstacles to healthy lives. At the same time, students are also dealing with people who have made a commitment to recovery, demonstrating courage and resolve in the face of daunting circumstances.”
It’s not your average rotation, Dr. Balderas said, so School of Dentistry faculty don’t treat it as one. Before students begin at the clinic, they are prepped about situations they may face. They’re shown the panic buttons affixed to hallway walls. They’re told to watch out for signs of “meth mouth,” the so-called calling card of the methamphetamine user, who often has decay in every tooth. They’re trained to look for the signs of a detoxing addict, whose behavior can swing radically from mellow to aggressive like a flip of a switch.
And they’re told they must not pre-judge their patients.
“It doesn’t matter what they look like, how they talk, what their language is. You treat them with respect. Members experiencing homelessness at Haven for Hope come from all walks of life,” Dr. Balderas said. “You’ve got people with master’s degrees and Ph.D.’s who were living on the streets.”
When the rotation is over, the students meet around a lunch table and reflect on the experience, led by Moshtagh Farokhi, D.D.S., M.P.H. FAGD, clinical assistant professor in comprehensive dentistry, who also works with the students at the clinic. What would they have done differently? How did they treat their most compromised patients? What was the hardest situation they faced?
Then they tour the Haven for Hope campus and get a glimpse at the lives their patients lead.
In essays, they write about their experience.
In her own words
“I assumed that the patients would be out of control and I would fear for my safety. Honestly, I am embarrassed that I felt nervous or scared about the idea of working on these patients. This impression completely changed over the course of the rotation. Many patients…did not appear to be any different from myself. This experience reminded me to look at patients as a whole and unique individual rather than letting the homelessness define the individual.”–Mary Grace Camp, student
Mary Grace Camp, a fourth-year dental student, readily admits she has thin skin. She was nervous about the rotation at the clinic, and expected the worst.
Two days into her rotation, while trying to get the medical history of a male patient, he began yelling, frustrated about the amount of time he had been waiting.
“I got a little upset, but I tried to stay professional and said ‘I would appreciate it if you don’t use that language with me,’” she said. She and Dr. Balderas calmed the patient, and he got through the appointment. But strangely for Camp, she said, she felt encouraged by the experience, not overwhelmed. She realized she was not helpless, but that many of her patients feel that they are. It gave her a better understanding of where they were coming from.
“Some of my patients were really thankful to be there and thankful to have someone take care of them,” she said. “I feel like every patient was just ecstatic to have treatment done.”
In most cases, they’ve never been taken care of before, said Dr. Farokhi. The U.S. Department of Housing and Urban Development reported that in 2014, San Antonio’s homeless population cited dental care as its highest need. Only 14 percent reported receiving the dental care they needed.
“They don’t have money. They don’t live in a warm house or apartment like you. They’ve been on the streets,” Dr. Farokhi said. “So when you give them attention and you’re polite and professional toward them, you are likely the first one that has done so. Then you do all this work. You take them out of pain, you remove their source of infection and you are courteous to them. That’s why they are so appreciative. You make a difference in their lives.”
Five years ago, the School of Dentistry faculty asked their pre-doctorate students if they would be interested in volunteering a half day once a week at the clinic. Their jobs would be similar to what is done routinely in the School of Dentistry’s eight clinics—exams, fillings and extractions. The response was overwhelming and unexpected. More than half of the fourth-year dental students signed up. The one critique faculty received repeatedly: One half-day a week wasn’t enough.
Eventually, the volunteer opportunity became a required weeklong rotation, funded through annual support from Methodist Healthcare Ministries. After collecting three years of reflection papers, Dr. Balderas said, it’s now obvious students want even more. Faculty are considering extending the pre-doctorate rotation to two weeks.
In the meantime, the school has expanded its services at San Antonio Christian Dental Clinic by adding residents in the advanced education in general dentistry program. Twice a week, they do more extensive dental work, such as root canals and surgical extractions. Dental hygiene students have also joined the rotation, providing cleanings and oral disease prevention education. Last year, 223 students, residents and faculty provided more than half of all dental services at the clinic.
“I see this as an opportunity for them in a tough environment to learn how to treat the most difficult behaviors in a positive manner,” Dr. Balderas said. “It’s a learning experience. Some of them go through a week without any major things, but they get to at least hear a story. They get the chance to validate someone’s life.”
[bgsection pex_attr_title="" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="" pex_attr_image="https://magazines.uthscsa.edu/mission/wp-content/uploads/sites/20/2015/06/dental-UTHSCSA-150414-1058-0943.jpg" pex_attr_imageopacity="1" pex_attr_bgimagestyle="static" pex_attr_titlecolor="ffffff" pex_attr_textcolor="ffffff" pex_attr_height="800"]
"I learned that it is not only
about dentistry but also about
spiritual care of the patients.
At the end, it is humanity
that we have in common.”—Jina George, fouth-year dental
student (seated at right).
[/bgsection]
Learning from experience
The rotation at San Antonio Christian Dental Clinic revealed a few surprises for Camp. One of them was how deeply she was touched by the stories she heard from her patients. They didn’t just give her a renewed appreciation for what she has, but they also reminded her that as a dentist, she’ll have a duty to help others who can’t help themselves.
“No one is immune to emergencies and disasters we can’t control that drain us of resources, financially and emotionally,” she said.
According to the clinic, an estimated 130 million people lack dental insurance in the U.S. Locally, less than half—41 percent—of Bexar County residents reported seeing a dentist in the past year. Compounding the problem, Bexar County and surrounding counties in the region are considered “dental deserts,” where the dentist-to-patient ratio is lower than that of the national average.
The patient load is higher for the students at San Antonio Christian Dental Clinic than at the clinics offered at the School of Dentistry. A typical day at the clinic can have up to five patients scheduled per dental student, plus emergencies. This is about two to three times higher than a typical day at the university’s clinics.
“For our part, the partnership [with the Health Science Center] extends our capacity for direct patient care, nearly doubling the numbers of underserved patients we treat,” Canseco said. The clinic has no paid dentists on staff, beyond its director of dental services. “The partnership guarantees a minimum threshold for capacity and assures a level of excellence on par with that of an academic health science center. And at a higher level, working with underserved patients contributes to the development of a social conscience for the students.”
These are lessons that can’t be fully taught in the classroom, said Dr. Farokhi. Life lessons. At San Antonio Christian Dental Clinic, it’s as real as it gets.
“I see more aha moments in these rotations than I ever do in the classroom,” she said. “But everything that is learned [at San Antonio Christian Dental Clinic] is true about all patients. Every patient has their own unique story. One shoe does not fit all.”
[bgsection pex_attr_title="" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-custom" pex_attr_bgcolor="" pex_attr_image="https://magazines.uthscsa.edu/mission/wp-content/uploads/sites/20/2015/06/dental-UTHSCSA-150414-1124-1083.jpg" pex_attr_imageopacity="1" pex_attr_bgimagestyle="static" pex_attr_titlecolor="" pex_attr_textcolor="" pex_attr_height="800"]
"As a dentist and leader of a dental team, it
is our professional responsibility to help all
patients in need of oral care. It is out duty
to help give back to the community that has
deemed us fit to hold the responsibility of
watching over their health care needs.- Adam Pfeifer, fourth-year dental student
(far right), discussing a patient case
with Vidal Balderas, D.D.S., M.P.H.
[/bgsection]

Asking 'why not?'

Photos courtesy of Kinetic Kids
It started with a simple question: Why can't kids with disabilities play sports?
In 2001, Tracey Fontenot and Kacey Wernli, physical therapists working at a local San Antonio hospital, wondered how they could get their young patients with physical and developmental disabilities to be active past their therapy sessions. What if they formed a baseball team, using the UT Health Science Center’s ball field? Would kids show up?
Ten did.
“Once we got out there, we saw the kids just come alive,” said Fontenot, ’96. “They felt so confident being part of a team. Their parents felt so happy to be able to watch their kids be able to do something active and to be able to be team parents.”
The physical therapists decided to continue the experiment. Over the next two years, the baseball group grew by 40 more players. In 2003, their experiment became an official nonprofit called Kinetic Kids.
Today, there are 1,800 special-needs children participating in 106 sports and recreation programs offered year-round throughout San Antonio.
Among the many programs offered are music, gymnastics, cheerleading, basketball, competitive swimming, flag football, golf and wheelchair tennis.
“It started with a question,” Fontenot said. “We asked ourselves ‘why not?’ and we did something about it.”
The majority of the staff, program directors and instructors are physical, occupational or recreational therapists. Of the 800 or so volunteers who help with classes each year, many are students from the Health Science Center’s physical and occupational therapy programs.
Although the sports and rec program isn’t considered traditional physical or occupational therapy, “we’re always thinking like therapists and are constantly working on maximizing their potential,” said Wernli, ’94. “We feel like the benefits of Kinetic Kids go beyond the health benefits. As they are out there participating in sports, they are also building relationships with people. They are having to take their turn and wait in line and do the things that other kids are doing in recreational sports.”
They’re also building confidence, Fontenot said.
“We hope that we’re building future community members,” she said. “Nobody here is going to play in the NFL or the MLB, but we’re building people who are confident and can be leaders because of the skills they have learned through their sports. Sports is just the mechanism by which they are learning all these different things.”
Kinetic Kids has become a full-time job for the founders. And it’s one they said they feel lucky to have.
“There is never a day where we’re dreading work. You just think of the kids you’re serving and the smiles on their faces and work is easy after that,” Fontenot said.
Just as there was a clear need for Kinetic Kids in San Antonio, there is a similar need in communities throughout the country, they said. Fontenot and Wernli would like to create a playbook that other organizations can use to bring similar programs to their cities.
“As people grow up and get married and start having families, we hope that they remember their childhood dreams of playing sports,” Wernli said. “I hope we inspire people to realize that every child has that dream [to play sports]. We can help make that dream come true.”









Alzheimer’s disease research gets multi-million dollar boost
Alzheimer’s disease is the sixth-leading cause of death in the U.S. There is no cure.
By 2025, the number of Americans age 65 and older with Alzheimer’s is projected to grow by 40 percent. Texas is expected to see an increase of nearly 50 percent in that same time.
“One in nine of us over the age of 65 is going to develop this disease,” said William L. Henrich, M.D., MACP, president of the UT Health Science Center. “The costs are incalculable.”
To help address the need, the Health Science Center is working to establish a comprehensive Alzheimer’s and neurodegenerative disease institute to offer patient care and support for caregivers while simultaneously developing effective therapies for early prediction, prevention and cures, Dr. Henrich said.
“We have a responsibility to lead the effort in providing a comprehensive, compassionate network of care for Alzheimer’s patients and their families,” he said. “We also must lead medical research to relentlessly search for new, much-needed therapies, including clinical trials, that will advance the field and offer promise for improved patient care, now and for the future.”
In less than a year, the university has raised nearly $30 million toward the creation of the institute. This vision was spurred by a $5 million gift from the J.M.R. Barker Foundation and a challenge to match the gift with additional community philanthropy and other external support for the institute.
“The Health Science Center has stepped forward to address a growing and serious health problem that is devastating to patients, and their families and loved ones, in this region and across the country,” said Ben Barker, board member of the Barker Foundation and member of the Health Science Center Development Board. “Our foundation is committed to investing in this vision for families.It touches all of us.
“If there is any area of science that needs a breakthrough, it is Alzheimer’s.”
The vision for the institute is to adopt the approach of a patient-centered medical home, grounded in comprehensive and continuous care for patients with Alzheimer’s, dementia, Parkinson’s disease and other neurodegenerative diseases. It will also offer social, psychological and other support programs for caregivers to continue providing care while also maintaining their own health and well-being.
Neuroscience research already makes up one-third of the science at the Health Science Center, Dr. Henrich said, and the institute would build upon that and add educational programs to provide more health care workers specializing in the care of patients with neurodegenerative diseases.
“Establishing the Alzheimer’s institute is of the highest importance to our university,” Dr. Henrich said. “We see a tremendous public health need on the horizon, and we recognize that we are positioned to address it in a substantive way.”
Texas is ranked third in the country in the estimated number of Alzheimer’s disease cases and second in the number of related deaths.
And as the Hispanic population continues to increase—Texas is projected to become a majority Hispanic state between 2025 and 2035—so too will the number of Alzheimer’s patients. Hispanics are about one and a half times more likely to have Alzheimer’s disease and other dementias than non-Hispanic whites.
“Texas and San Antonio are right in the sights of this disease,” Dr. Henrich said. “This gift from the Barker Foundation, and the many others we have received for this critical endeavor, will allow us to provide the research and compassionate and expert care to address the critical need for the growing number of families and patients who are facing this serious and challenging condition.”