And then there was light
Pat Johnson vividly recalls his near-death experience after a boating accident on the Blanco River nearly six years ago. He speaks of that day in reverential tones, of being “in the presence of God” and “at the edge of heaven.”
And he recalls telling his doctor about the experience.
“He basically laughed at me,” Johnson said. “He chuckled and said, ‘Oh, it’s just your frontal lobe shutting down that causes you to have this euphoric feeling and you hallucinate.’ I told him that, no, this wasn’t a hallucination, this wasn’t a dream. ‘It was as real as me standing here talking to you.’ At that point I thought, I don’t care what anyone tells me.”
While near-death experiences are common, so too is the reaction by Johnson’s physician, said Deborah James, M.S.N, RN, CNS, CCRN-K, a clinical assistant professor in the School of Nursing and recognized expert in end-of-life care and near-death experiences.
James, who in 2009 co-authored and co-edited the first compilation of research on the subject, Handbook of Near-Death Experiences: Thirty Years of Investigation, said one in three people who have a close brush with death report a near-death experience.
And James is on a mission to make sure health care professionals, nurses in particular, know how to listen and respond when a patient recounts such a profound experience.
 Over her decades-long career, most spent in intensive care units or other critical care settings, James has met and listened to dozens—if not hundreds—of near-death experiencers, or NDErs. All the stories are different, but there are many common threads.
Over her decades-long career, most spent in intensive care units or other critical care settings, James has met and listened to dozens—if not hundreds—of near-death experiencers, or NDErs. All the stories are different, but there are many common threads.
Johnson’s story begins when he was kayaking with a friend on a swollen river. He was suddenly sucked into a pipe underneath a low-water crossing. Under water, he fought to pull himself out but couldn’t. He was drowning, and soon lost consciousness.
Still, he said, “I felt like I knew where I was at, and I was in a good place. And I thought, I haven’t been that great a person, but I felt like I was in heaven, in the presence of God.”
He sensed “a multitude” of souls around him.
“I didn’t see them but I felt a part of them. I knew they were there.”
And then there was light, “like looking into a kaleidoscope,” Johnson said. “I wanted to get to the light, go to the light.” He was at peace, surrounded by love. “It was beautiful. If I had stayed there, I would’ve been fine with it.”
But somehow the current swept Johnson through the pipe and deposited him downstream, where his friend pulled him to safety and resuscitated him.
As with Johnson’s experience, a common thread is the bright light at the end of a tunnel or hallway, and an extraordinary sense of love and serenity.
“This is not any laughing matter,” James said. “This is not one of those things that people dream up. This is not a dream.”
Years ago, James said, a patient in ICU became irate after he was resuscitated.
“He said, ‘I can’t believe you people made me come back.’ And everybody is like, ‘We did our job. He must be confused.’”
It’s not unusual, she said, for health care professionals and others to consider NDErs to simply be confused, disoriented or trying to get attention.
“What happens many times is those patients get medicated,” James continued. “Health care providers will often order medications because they think the patient is psychotic. Often veterans are treated as if they’re suffering from PTSD.”
So it’s normal for NDErs to be a bit leery of communicating the details of what happened.
“Some people think you’re crazy,” said Johnson, the near-drowning victim. “Almost immediately you develop a sense of who you can talk to about it and who you can’t.”
And if a near-death experiencer is afraid to tell his story or it’s casually dismissed, the person feels rejected, becomes more isolated, more apt to question the experience, and more prone to have self-doubts and fears. They may keep the experience bottled up inside for years.
James, who teaches a variety of courses at the Health Science Center, introduces near-death experiences and the proper response from health care providers whenever she can: while talking about anything from end-of-life or palliative care and hospice to patients coming out of resuscitation.
“As nurses,” James said, “we should listen without judgment. You can tell the difference between someone who is confused and really struggling and someone who’s had a near-death experience.”
More and more health care professionals are responding positively, James said. So are students.
Brittany Jasso, a nursing student who will graduate in May, said nurses should always be open to what near-death experiencers are saying.
“You should ask them to tell you more, like, what did you see, what did you feel,” she said. “I’m not there to minimize their feelings. I’m not there to judge them.”
Despite the skepticism of his doctor, Johnson continues to be enthusiastic about sharing his story, meeting others with similar experiences and seeking a deeper meaning as he gets on with life. And he thinks health care providers are crucial, especially in the beginning, in that search for meaning.
After all, he said, “a near-death experience is more about living than it is about dying.”

Healing in flight
Photo courtesy of the U.S. Army. Photo by Sgt. Duncan Brennan, 101st Combat Aviation Brigade public affairs.
Getting wounded soldiers the fastest, most skilled emergency medical care possible and transporting them to forward units or hospitals has long been a priority in warfare. To that end, the Army turned to the Long School of Medicine and its expertise in emergency care.
After a yearlong pilot project in 2011, the Department of Emergency Health Sciences was selected by the Army in 2012 to train all Army flight medics. A five-year contract calls for the university to provide four paramedic certification courses and four critical care transport courses per year for flight medics. This year, due to the success of the program, the department will offer six courses.
It’s a charge that Lance Villers, Ph.D., LP, associate professor and chair of the department, doesn’t take lightly.
“All of these soldiers are EMTs who were trained at Fort Sam,” Dr. Villers said, explaining that San Antonio’s Fort Sam Houston is the center for all medical training for the Army. “Many of them have been deployed and have combat experience. Then all of the designated flight medics for the Army are brought back here for our training.”
Intensive classroom instruction covers anatomy/physiology, patient assessment, advanced airway procedures, cardiovascular emergencies, medical and trauma emergencies, EMS operations, hospital clinicals and EMS field practicums.
“When they finish our program, they’re prepared for national certification for paramedic,” Dr. Villers said. And then immediately “they start an eight-week, critical care transport program. This is even more advanced training that prepares them for a national certifying program to be flight paramedics.”
Rotations include the operating room for airway procedures, various intensive/critical care wards, the burn unit, cardiac catheterization lab, neonatal intensive care unit and pediatric intensive care unit, and obstetrics for delivering babies. This phase emphasizes the development of critical thinking skills.
All clinical time is done at civilian hospitals and specialty clinics in the San Antonio area.
Lt. Col. Neil B. Davids, M.D., LTC, Critical Care Flight Paramedic Program director at Fort Sam Houston, said the program's quality is reflected in its high first-time pass rate on the National Registry Paramedic certification exam—nearly 20 percent higher than the national average.
“Getting the clinical experience, both in the hospital and riding out with various EMS agencies, has been crucial in meeting our goal of having paramedics with critical care training [available] to the fighting force,” he said.
Dr. Villers finds significance in the work his department does for the Army.
“This training makes a difference for soldiers,” he said. “Once these soldiers complete our training, they go right back out to their deployments, many to a combat zone. And they’ve been given a new set of tools, of knowledge, to save people’s lives. We’re proud to be part of that.”

The 'lost' population
PHOTOS BY JOEL SPRING
Student-run clinic brings health care to those fleeing violence and persecution

In the triage area, second-year medical student Fadi Al-Asadi, who was born and raised in Iraq and whose first language is Arabic, bends down to try and wake a sleeping toddler in a stroller. “Bon jour,” Al-Asadi says jovially to the French-speaking child from Cameroon in West Africa.
Across the way, nursing student Christina Potts is busy processing new patients. There’s a three-generation family from Burma, followed by a couple and their children from Bhutan. Next up is an elderly, white-bearded man from Iran wearing a woven, white prayer cap. The “waiting area”—chairs lined up and down the hallways—is crowded with refugees, each with a personal story of fleeing violence, persecution and war. The place is teeming with sound and color, the cadences and rhythms of world languages and bright ethnic dress from Africa, the Middle East and the Indian subcontinent.
And they keep coming through the doors of the makeshift clinic at St. Francis Episcopal Church on Bluemel Road, near the South Texas Medical Center. Sniffling babies, stooped men and stoic women, all seeking health care.
This is a San Antonio health clinic like no other. It is the Health Science Center’s student-run, free San Antonio Refugee Health Clinic, a blessing for refugees and a teaching tool without parallel for the students who volunteer.
Back in triage, Al-Asadi, who was a teenager in Baghdad when the U.S. invaded Iraq in 2003, is moving from patient to patient, listening, learning, treating. He spent a year in Syria as a refugee himself before coming to the States in 2008, and so has “a personal connection” to the patients.
“Compassion is about 90 percent of the whole deal,” he said.
[bgsection pex_attr_title="" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-dark" pex_attr_bgcolor="000000" pex_attr_image="" pex_attr_imageopacity="1" pex_attr_bgimagestyle="static" pex_attr_titlecolor="ffffff" pex_attr_textcolor="ffffff" pex_attr_height="150"]
Governments create borders. Diseases do not follow those borders. If we’re not educating our students in global health, we’re doing a great disservice.”
—Andrew Muck, M.D., medical director for the Refugee Health Clinic
[/bgsection]
A helping hand
The Refugee Health Clinic, which operates weekly, began in 2011, building on a School of Nursing effort. It is one of five student-run clinics that operate through the Center for Medical Humanities & Ethics, and is by far the most interprofessional with medical, dental, nursing and physician assistant students and faculty advisers.
It is estimated that 4,000 to 5,000 refugees live in a small area off Wurzbach Road in northwest San Antonio, within three miles of the Health Science Center. About 1,000 arrived in 2014 alone. They hail from dozens of countries, including Iraq, Cuba, Burma, Afghanistan, Iran, Bhutan, Congo, Somalia, Eritrea and Ethiopia.
Most refugees who are resettled in the United States are given temporary health benefits by the federal government that typically run out after six to eight months. Many of those who rely on the student-run clinic have no insurance, few resources and are without regular medical care. The Refugee Health Clinic plays a vital role in filling this gap, treating an estimated 500 patients a year.
“It’s really a lost population,” said Victoria Petty, one of the nursing student leaders at the clinic. “When you think of refugees, you think of New York or Miami. You think of these big portals of the U.S., not San Antonio. But we really have a population here that’s not even recognized.”
Patients mirror those from any outpatient clinic, with general health concerns, said Al-Asadi, one of the medical student leaders.
“We get patients who are there for back pain, for the flu, for uncontrolled diabetes, for hypertension, for rashes, for dental problems. We even get pediatric cases,” he said.
The students, under the guidance of faculty mentors, provide basic care and referrals, all at no charge.
“The point of the clinic is not to always have them come back to the clinic, because it’s an outpatient clinic,” Al-Asadi said. “The point is to treat them at that moment and try to get them linked to the health care system here in San Antonio. If they don’t qualify for the [Affordable Care Act], we try Carelink, a financial assistance health care program through University Health System. And usually we’re successful with that.”
Listening, learning, treating

The refugee clinic provides unique challenges and opportunities for the future health care providers. One is the interprofessional nature of the setting. Teams are made up of a medical student, a nursing student and a dental student. They all observe each other’s role in the patient’s treatment and report as a team to their faculty advisers.
“I feel like I’m applying nursing school [lessons] even before I’ve graduated,” said Petty. “You learn the behind-the-scenes of a clinic, you learn how doctors interact with patients, how dentists interact. It’s all-encompassing. You get more information there than you’d get in a regular classroom.”
Students are able to learn from each other, said Peggah Hemmat, a fourth-year dental student and first-generation Iranian-American.
“As a dental student, I’ve learned so much about the medical aspect and how to interview patients and what questions to ask,” she said.
“I remember a patient who had periodontal disease, bone disease. And they had no idea what that was. We had to sit with them and explain why this is happening, what are some risk factors and how do we make sure you don’t lose all your teeth. Not only was it a learning experience for the patient, it was a learning experience for the nursing and medical students.”
A particular test for the students comes with the nature of the patient population itself.
“One of the greatest challenges is dealing with so many different cultures, so many different languages,” said Eden Bernstein, one of the medical student leaders. “We try to have adequate interpreters, but a lot of times we have to improvise and be very patient with the patients that we see. There’s not really an easy answer, it’s just kind of being resilient and focusing on the task at hand.”
Many of the students, as well as the faculty advisers, have some sort of international background or experience, and many are bilingual. There are Arabic speakers such as Al-Asadi, the medical student. Hemmat, the dental student, speaks fluent Farsi. Alizain Maneshia, a nursing student and native of Pakistan, speaks Hindi. Others speak French and Spanish.
In some cases, one member of a patient’s family speaks enough English to translate. But still, at times, interpreters have to be hired. Aside from the language differences, many refugees have had little experience with health care and find it difficult to describe symptoms or illness progression.
[bgsection pex_attr_title="" pex_attr_subtitle="" pex_attr_undefined="undefined" pex_attr_style="section-dark" pex_attr_bgcolor="000000" pex_attr_image="" pex_attr_imageopacity="1" pex_attr_bgimagestyle="static" pex_attr_titlecolor="ffffff" pex_attr_textcolor="ffffff" pex_attr_height="150"]
You don’t have to do mission trips in another country to learn about the world.
The world is here in San Antonio.”
—Moshtagh R. Farokhi, D.D.S., M.P.H., clinical assistant professor in comprehensive dentistry and dentistry adviser for the Refugee Health Clinic
[/bgsection]
Stepping out of the box
If the cultural challenges are steep, the gratification is abundant, the students agreed.

“Every time I leave the refugee clinic, I know that I’ve impacted this population just a little bit more,” Hemmat said. “Every one of these cultures is very family oriented. So if you tell them just a little about oral hygiene or teach them how to take care of their teeth, it will permeate through the rest of their [family circle].”
Bernstein, the medical student, contrasted his experiences at the clinic with classroom work.
“Going through the curriculum for the first years of medical school—it’s the preclinical medicine where we focus on the disease process, on the science,” he said. “It’s very textbook-oriented learning. So any time that I’m able to step out of that little box and glimpse what I’ll eventually see as a doctor and how I can potentially make an impact in the future, it’s invigorating and exciting.
“Every once in a while I see a patient and I’ll refer them out to receive care from a different place or we send them to get labs at University Hospital, and we follow them up at the next clinic and I see that the treatment that we gave them worked and they’re better. It’s very refreshing to feel that you’ve made this impact.”
Petty, the nursing student, pointed to the inherent altruism in health care fields.
“I wanted to be a nurse because I like pus and broken bones and blood,” she said, only half-jokingly. “And it’s exciting. And at the end of the day, whether it’s something as outrageous as that or something as simple as helping a Nepalese man to overcome the flu at our clinic, you’re helping someone.”
Al-Asadi remembers a refugee who came to the clinic suffering from severe anemia. He was able to diagnose it and get her the proper treatment.
“I felt happy,” he said, “because I thought that was the gratification I was looking for. To make people feel better and to feel gratified, I think that’s part of the payment. It’s not necessarily financial. It’s a humanitarian profession, and we all signed up to serve people. And we should keep that always in sight.”

Waist not
Diet sodas linked to waist gain
You could search all day in Sharon Fowler’s kitchen and pantry and there’s one thing you’d never, ever find: diet soda.
“Absolutely not,” said Fowler, M.P.H., adjunct faculty in the School of Medicine at the Health Science Center.
Fowler was the lead author of a paper published in the Journal of the American Geriatrics Society that described how consuming diet sodas was linked to subsequent increases in waist size among people 65 and older: The more diet sodas they drank, the more their waist size grew over the next decade. Data for the study came from the San Antonio Longitudinal Study of Aging (SALSA), led by Helen P. Hazuda, Ph.D., senior author and professor of medicine at the Health Science Center. Ken Williams, M.S., P.Stat., adjunct faculty in the Long School of Medicine, co-authored the paper and performed all analyses reported in it.
“There’s a heated debate about whether this is a causal relationship,” Fowler said. “It’s my personal opinion that it is.”
One of the explanations is that the artificial sweeteners themselves affect the metabolism, Fowler explained. If a person tastes something sweet, it’s not just the brain that absorbs the information; so do other parts of the body. When the body registers sweetness, it ramps up to deal with sugar. But if there isn’t real sugar present, the body doesn’t know how to handle it.
“It’s kind of like crying wolf,” she said, and can lead to metabolic dysregulation.
To make matters worse, Fowler said, one of the most dangerous places you can gain weight is your middle, because increasing waist size is linked to increasing visceral fat and an increase in inflammation, which is tied to the increased risk of arthritis, diabetes, cancer, heart attack, Alzheimer’s disease and other major medical problems.
What’s next for Fowler? She’s currently pursuing her doctorate in epidemiology and plans to continue her research on artificial sweeteners.
“What I am most concerned about is when women are pregnant and they’re using diet sodas, or consuming artificial sweeteners in other ways,” she said. “What is happening to their unborn child? There are a number of people who have reported neurological problems when they themselves have taken certain artificial sweeteners—brain fog, memory loss. I want to look at whether the unborn child is at increased risk of developing neurological problems when the mother has been exposed to artificial sweeteners. To me, that would be infinitely worse than gaining or losing a few pounds.”

Drawing it out

and an alumna of the School of Nursing.
Zyren Lopez just can’t tolerate cats. “Cats and dust,” he said in a polite whisper.
In the second grade, Zyren recalled, “I started getting really sick. My chest was hurting and it was hard to breathe, so I went to the nurse and she called my mom. And they wanted to take me to the doctor. They wanted to rush me to the hospital.”
Zyren was soon diagnosed with asthma, a chronic lung disease that inflames and narrows the airways, making it hard to breathe. Asthma affects one in 10 people, including an estimated 7 million children in the United States.
Now 11 and soon to be a fifth grader at Driggers Elementary on San Antonio’s northwest side, Zyren considers himself a normal kid, albeit one who must be aware of symptoms and triggers and who takes daily long-term asthma control medications.
“I am a registered respiratory therapist certified in asthma education and I’m an artist. I believe Asthma2Art is a great way for children to express what it feels like to live with asthma,” said Hart, assistant professor and director of clinical education in the Department of Respiratory Care in the School of Health Professions.
The program for children who have already been diagnosed with asthma has two components, Hart explained: education and artistic expression. First, she and a respiratory care team go to a school and provide asthma management education to the students with asthma. Three education stations are set up for the students to rotate through during the program, each focused on a different subject.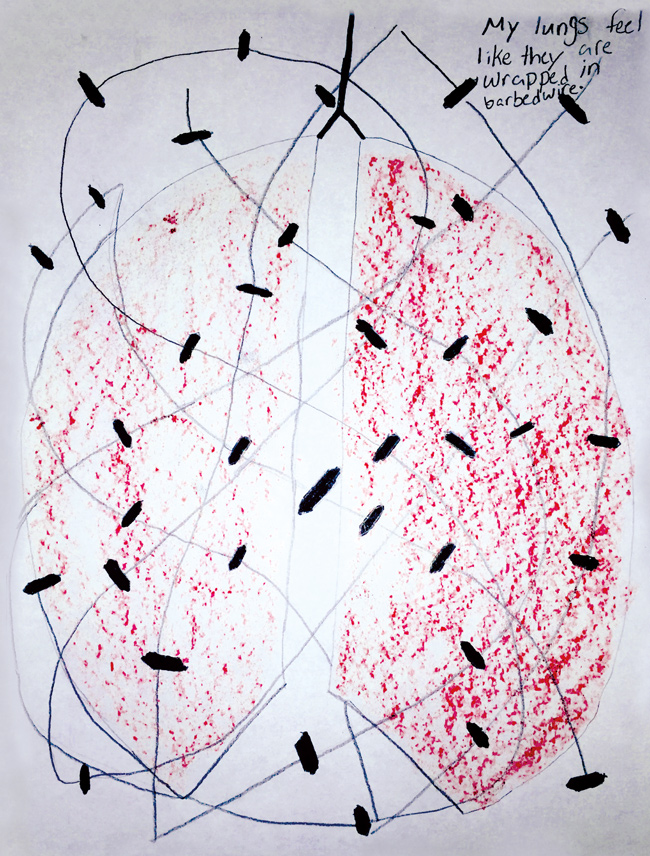
“The ‘What is Asthma?’ station teaches the students how the lungs work and signs and symptoms of asthma,” Hart said. “Another station is focused on asthma triggers. Students identify their own asthma triggers, how these triggers make their asthma worse, and which triggers can cause them to have an asthma attack.”
Common triggers include allergens such as pollen, dust mites, cockroach droppings and mold, she said. Frequently, triggers are in the schools themselves, where carpeted libraries and stacks of books can gather dust mites, and water leaks in the ceiling or beneath sinks can accumulate mold.
After the stations comes the art.
 “Some kids choose to draw pictures of what triggers their asthma,” Hart said. “Others draw pictures of being totally isolated indoors and unable to go outside with friends, because that’s the way they’ve lived. The pictures I most enjoy seeing are the ones they create of them participating in the fun activities they enjoy when their asthma is controlled.”
“Some kids choose to draw pictures of what triggers their asthma,” Hart said. “Others draw pictures of being totally isolated indoors and unable to go outside with friends, because that’s the way they’ve lived. The pictures I most enjoy seeing are the ones they create of them participating in the fun activities they enjoy when their asthma is controlled.”
Kathryn Cruz, RN, is the school nurse at Driggers Elementary and an alumna of the Health Science Center’s School of Nursing. About 100 of Driggers’ 640 students have been diagnosed with asthma, and most participated in the Asthma2 Art program in January, she said. Cruz called the artwork the students created meaningful and amazing.
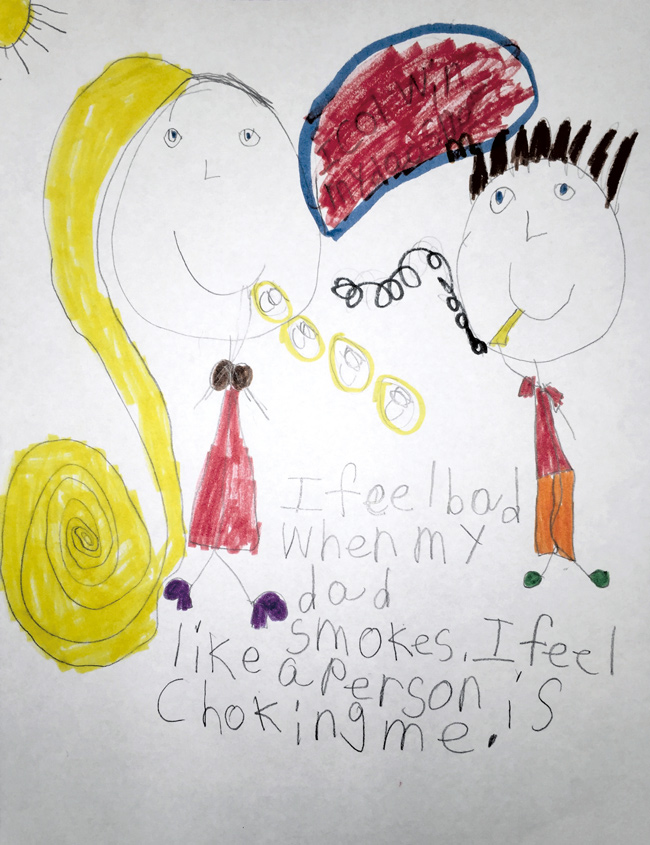
“One child [expressed] that during an asthma attack it felt like barbed wire, just very tight and painful on his chest,” Cruz said. “Another little girl who was a second grader drew a very nice picture of her and her dad there in a house, and the dad was smoking, and she said, ‘Dad, please stop smoking. I can’t breathe.’ And I was just very taken aback by that.”
Tobacco smoke is especially bad for kids who have asthma, Hart said.
“It’s very important for adults to know that just being around someone after they have smoked a cigarette can trigger an asthma attack. Even emotions such as crying hard or laughing can trigger asthma,” she said.
Since children spend most of their days in school, Hart and her team surveys the physical condition of the school and identifies potential asthma triggers. They recommend ways to maintain asthma-friendly classrooms and train teachers and staff to recognize signs and symptoms of asthma and respond properly to a child having an asthma attack.
“During the cold and flu season, lots of children come to class coughing and with runny noses, both classic warning signs of asthma,” she said. “Knowing in advance which children in the classroom have asthma may reduce the risk of an emergency situation. Otherwise, it may be missed.
“There are tragic instances where a child has died at school from an asthma attack. It was either not recognized as an emergency or the school did not have the medication readily available to treat the child soon enough. Having asthma action plans in place for the school to follow for each child and having school staff trained in asthma emergency management is key to preventing this from ever happening here in our schools.”
Asthma2Art allows students, like Zyren, to articulate their fears and frustrations about the disease. Indeed, art therapy has proven to decrease anxiety and increase quality of life for children with persistent asthma, according to a study from National Jewish Health. To date, six San Antonio schools have participated in Asthma2Art aided by a grant from the Environmental Protection Agency.
Zyren, who wants to be an artist, said he enjoyed drawing a dreaded cat in the Asthma2Art program “because I could tell what’s going on with my asthma.”
All artwork is judged by local artists and the winning artwork is published in a calendar.
“We’ve seen incredible pictures that speak louder than words, very emotional pieces describing what it feels like to live with asthma,” Hart said. “We are hoping through Asthma2Art to raise asthma awareness and offer tips to others about managing their asthma better.”

Professor emeritus continues life’s work through endowment
 Rajam Ramamurthy, M.D., may have been born and raised in India, but she’s grown fond of a particular American idiom.
Rajam Ramamurthy, M.D., may have been born and raised in India, but she’s grown fond of a particular American idiom.
“I believe you should put your money where your mouth is,” she says flatly.
Dr. Ramamurthy, professor emeritus in pediatrics, has a long history of giving back financially to the Health Science Center, where she has worked since 1977. Her latest gift of $100,000 established the Dr. Rajam Ramamurthy Endowment in Neonatology to support educational activities related to research on prematurity and premature infant care.
As a renowned neonatologist, Dr. Ramamurthy’s endowment is a continuation of her life’s work.
“When I took over the premature infant development clinic in 2000, one of the things I felt was that there was no educational activity in San Antonio or in most of South Texas for professionals who are helping these infants, such as physical therapists, speech therapists, occupational therapists, even physicians, pediatricians,” she said.
Once discharged from the neonatal intensive care unit, premature babies “were put in the mix of normal, full-term newborns…But these babies are extremely vulnerable, very delicate, and at least for the first few years of their lives they need very specialized, developmental care.”
The endowment will be used to educate those in the region about the importance of specialized care for premature infants. To that end, a portion of it was used to host the university’s first Rajam Ramamurthy Lectureship in Premature Infant Development in February, which featured Tonse Raju, M.D., medical officer of the National Institute of Child Health and Human Development in the National Institutes of Health.
The Ramamurthy family began giving to the university in 1996. In that time, their donations have surpassed $154,000, and have supported various university initiatives and programs including student scholarships and endowments for research and education. In 2013, the family created the Dr. Somayaji Ramamurthy Professorship Fund in Pain Management, named for Dr. Rajam Ramamurthy’s husband, Somayaji Ramamurthy, M.D., a professor of anesthesiology.
Faculty gifts are an especially powerful example of philanthropy because of what they already contribute to the university in their time and brainpower, said William L. Henrich, M.D., MACP, president of the Health Science Center.
“Our faculty is the engine that drives the missions of our university, and giving fuels the engine,” he said. “They see firsthand the impact of what is accomplished here, and they know the difference gifts can make. It is inspiring to see faculty invest in the future of our university through their own philanthropy.”
Faculty, by and large, do not amass great wealth, Dr. Rajam Ramamurthy said. Giving back takes a commitment. The first family endowment began on her and her husband’s 25th wedding anniversary when they asked their friends to forgo giving gifts and buy artwork instead, the proceeds of which funded the endowment.
“Gifts like these help us all see the good one person—one family—can do,” Dr. Henrich said.
Although retired, Dr. Rajam Ramamurthy plans to continue research in prematurity and stay involved at the Health Science Center. And she’ll keep on giving.
“My experience is you need to support things you believe in,” she said. “And it’s very important to do these kinds of activities so that these efforts can be sustained.”